Download to read offline

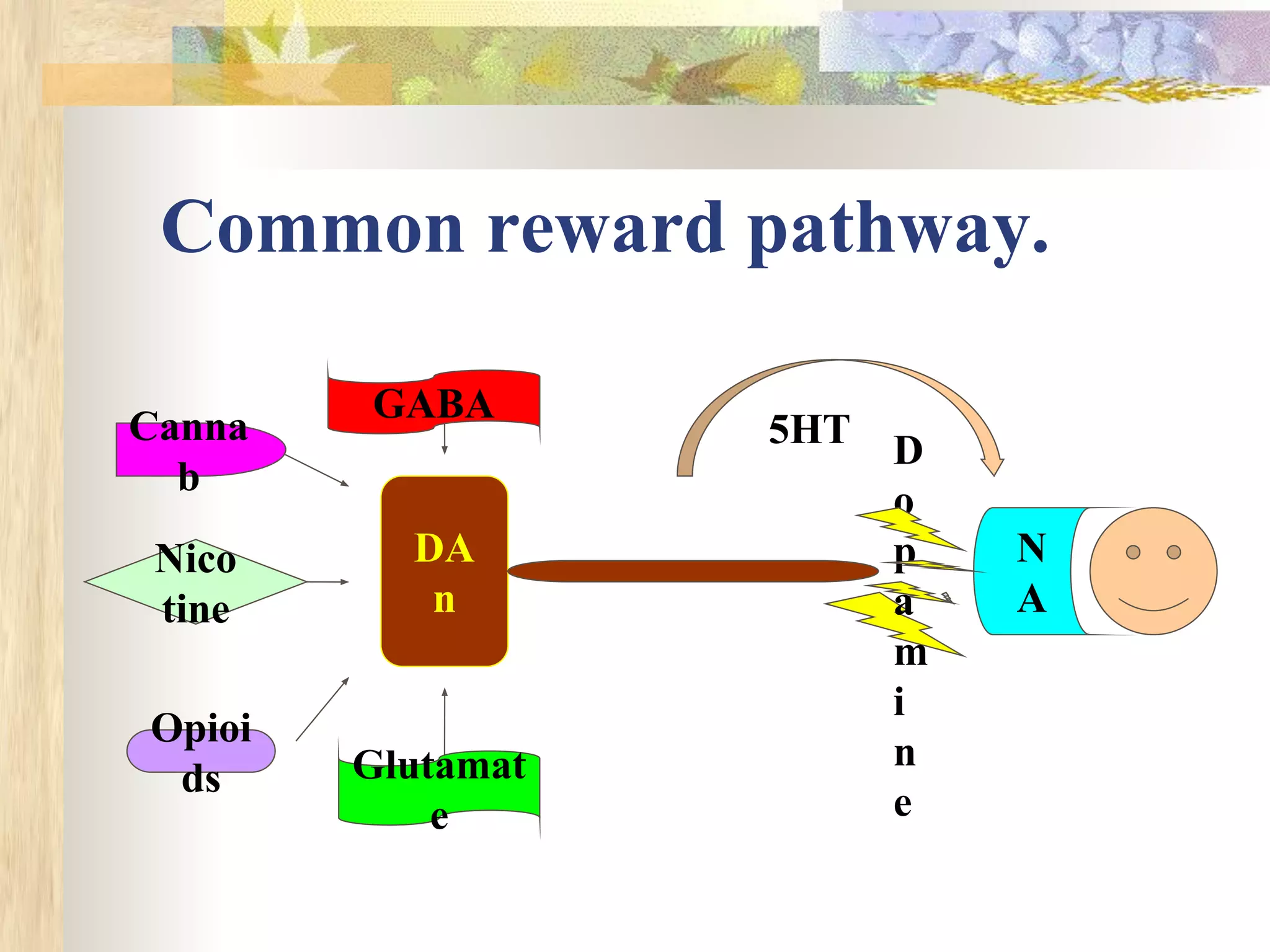
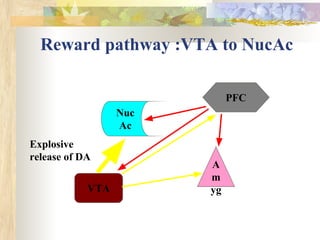
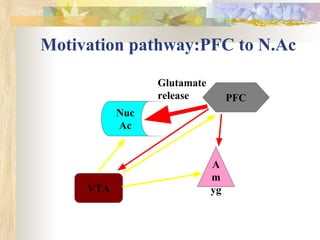
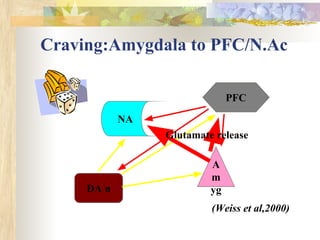
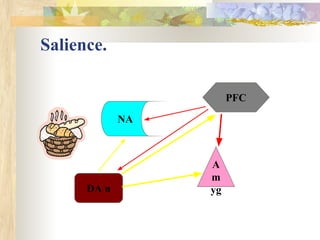
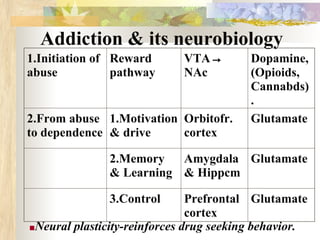
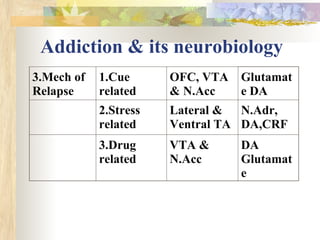
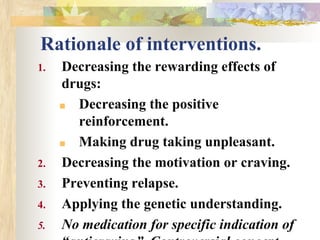
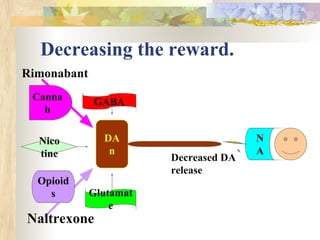
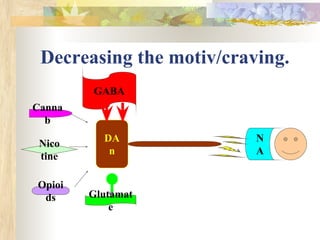


The document discusses the neurobiology of addiction and rationale for pharmacological interventions. It describes the common reward pathway in the brain activated by drugs like dopamine, opioids, nicotine, and cannabinoids. It outlines three stages in the addiction process - initiation due to reward, development of dependence and motivation, and mechanisms of relapse. It then provides rationale for decreasing reward, motivation/craving, and preventing relapse by targeting specific neurotransmitter systems. Several pharmacological agents are proposed to work through these mechanisms, such as decreasing dopamine, modulating glutamate and GABA, and regulating serotonin. Combination therapies and targeting specific subtypes of alcoholics are also suggested.






































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















