
More Related Content
Similar to Adrenergic agonists (Sympathomimetic drugs).
Similar to Adrenergic agonists (Sympathomimetic drugs). (20)
More from AhmedAbdElMoniem35
More from AhmedAbdElMoniem35 (20)
Recently uploaded
Recently uploaded (20)
Adrenergic agonists (Sympathomimetic drugs).
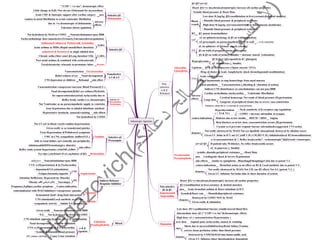
- 1. Adrenergic Agonists Adrenaline Epinephrine Noradrenaline Norepinephrine β1>β2>α1>α2 Heart: β1(+ve ino,chrono,dromotropic) increase all cardiac properties Low dose<0.1µg/kg :β2(vasodilatation in liver,coronary&skeletal muscles) Blood vessels High dose>0.1µg/kg :α1(vasoconstriction in skin&mucous membrane) RT β2: potent bronchodilator GIT α1 on sphincters(closing) & β2 on walls(relaxation) α2 presynaptic on parasympathetic nerve to wall A.Ch. (relaxation) UT α1 on sphincter of detrusor muscle (closing) Hyperglycemia β2 in liver (glycogenolysis &↑ glucagon) α2 in pancreas (↓ Insulin) Lipolysis β1 & β3 in adipocytes (↑lipase enzyme ↑FFA) Uses Drug of choice in Acute Anaphylactic shock (bronchspasm&vasodilatation) Acute cardiac arrest Local haemostatic to stop hemorrhage from nasal mucosa Local anesthetic Vasoconstriction (↓bleeding & ↑duration of action) Adverse effects β2 & β3 on walls of urinary bladder = detrusor muscle (relaxation) β2 on walls of pregnant uterus (relaxation) Indirect CNS disturbances as catecholamines can not pass BBB Cardiac arrhythmias (tachycardia) Ventricular fibrellation Gangrene of peripheral tissues due to severe vaso constriction Cerebral hemorrage Net result of blood pressure (Hypertension) Large dose Pulmonary edema due to +ve inotropic & vasoconstriction contra-indications No.& sensitivity of β receptors (up regulation) COMT = increase adrenaline in synapse Beta blockers as in low dose, vasoconstriction occurs (Hypertension) Cocaine as it prevents reuptak=incrase adrenaline&exaggerated CVS action Diabetes due to low insulin Hyperthyroidism ( ↑ T3 & T4 ) Non selective α & β Releasers α1>α2>β1 α 1(vasoconstriction &↑↑ Reflex bradycardia”- vechronotropic”)&β1(weak+veinotropic) uses Cardiogenic shock & Severe Hypotension contra-indications Bronchial astma as no effect on B2 & Local anethetic due to potent V.C. side-effects similar to epiniphrine , Blanching&Sloughingof skin due to potent V.C α2 in pancreas (↓ Insulin) Kinetics Not orally (destroyed by MAO) Not I.M. (no B2 effect) Not S.C.(potent V.C.) Given I.V. Infusion Not bolus (due to short duration of action) HOCM = IHSS Kinetics Given I.V. bolus in ICU not I.C.(still V.D.) I.M.(B2=V.D.) Inhalation(local B2 broncodilatation) Not orally (destroyed by MAO) Not eye dps(little absorption& destroyed by alkaline tears) Angina If patiend take M-blocker, No reflex bradycardia occurs Non selective β1 & β2 Isoproterenol Isoprenaline Heart: β1(+ve ino,chrono,dromotropic) increase all cardiac properties β2 (vasodilatation in liver,coronary & skeletal muscles) systolic, diastolic,peripheral resistance Heart Rate Systolic&Heart rate Diastolic&peripheral resistance Kinetics Destroyrd by COMT NOT by MAO Acute bronchial asthma & Heart stimulant in ICU uses Dopamine Low dose: D1=vaodilatation=incrase renal&visceral blood flow Intermediate dose: β1 ("↑COP=+ve ino"&chronotropic effect) High dose: α1 ( vasoconstriction=Hypertension ) Given orally & inhalation Shock due to myocardialinfraction,Renal failure,Trauma correct tissue perfusion rather than blood pressure uses kinetics Destroyed by COMT&MAO into homovanillic acid Given I.V. Infusion (short duration&dose dependent) Selective β1 Dobutamine "↑COP = +ve ino", dromotropic effect Little change in H,R,=Not elevate O2demand for myocardium uses Acute CHF & Inotropic support after cardiac surgery Adverse effects caution in atrial fibrillation to avoid ventricular fibrillation Tolerance (down rgulation) Selective β2 Ritordine SABA Salbutamol=albuterol, Pirbuterol& terbutaline Acute asthma as MDIs (Rapid onset&Short duration) due to +ve dromotropic of dobutamine LABA salmeterol & formoterol as single inhaled dose Chronic astha (Slow onset &Long duration=12h) Tocolytic(uterine relaxant) in premature labor Noct urnal asthma & combined with corticosteroids Noncatecholamines=pass BBB Not hydrolized by MAO or COMT Tachycardia(large dose=nonselective)Tremors,Tolerance(downregulation) Nonselective α 1 & α 2 Oxymetazoline Nasal decongestant Relief redness of eye Vasoconstriction side effect Rebound CNS depression at children Selective α1 Phenylephrine Methoxamine Vasoconstriction=vasopressor=increase Blood Pressure(I.V.) Nasal decongestant,Relief eye redness,Mydriatic Reflex brady cardia (-ve chronotropic) for supraventricular(atrial) tachycardia due to Not Ventricular as no parasympathetic supply to ventricles side effects Hypertensive headache, nausea&vomiting Clonidine Brimonidine Selective α2 Presynaptic Eye dps (↓mydriasis of α1↓aq.humor of β2) Not I.V.(α2 in blood vessels=sudden hypertension) Given orally or as transdermal patches Treat Hypertention &Withdrawal symptoms VMC in CNS, sympathetic outflow(N.E.) side-effect sidation,salt&H2Oretention(give diuretic) Reflex renin system=hypertensice crisis متبطلوش فجأة Safe to renal failure (act centrally not peripherla) Amphetamine CVS: α (Hypertension) & β (Tachycardia) CNS dopamine&N.E.(stimulation) Fatigue,Insomnia,Appetite use Attention Defficiency Hyperactivity Disorder Narcolepsy Contra-indication Pregnancy,Epilipsy,cardiac proplems Obesity بالش لمرضى القلب Tyramine Noncaticholamine=pass BBB addictive contraindicated with MAO Inhibitors=vassopressor episodes Cocaine CNS stimulant&Local anethetic as eye dps Inhibit N.E.reuptake sympathetic activity Mixed Ephedrine Pseudoephedrine Noncatecholamines=pass BBB Not hydrolyzed by MAO or COMT Given orally CNS stimulant opposing hypnotic effect of antihistamine α & β Agonists broncho dilatation N.E. Nasal decongestant Systolic & Diastolic blood pressure CVS: α (Hypertension) & β (Tachycardia) Cause Urine retention OTC common cold drugs Indirect Releaser Reuptake Inhibitor fermentated food= drug-food interaction Diastolic blood pressure & peripheral resistance Diastolic blood pressure & peripheral resistance Systolic blood pressure & Heart Rate Not hydrolized by COMT treat hypotension due to inhaled halothane anethetic over dose Anginal pain, tachycardia, nausea & vomiting