Download as PDF, PPTX


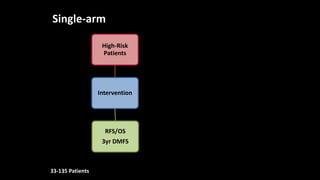
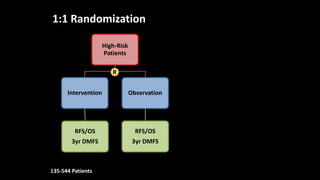
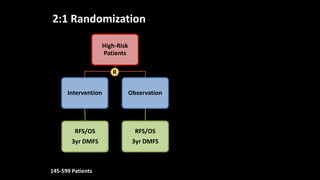
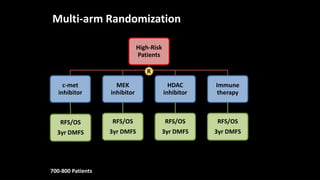





The document presents an overview of adjuvant therapy and clinical trials for melanoma, discussing their definitions, trial designs, and specific interventions for high-risk patients. It highlights various treatment approaches including interferon, ipilimumab, and peptide vaccines, along with the challenges faced in patient enrollment and compliance. Current and future options for adjuvant therapies are also mentioned, emphasizing the significance of clinical trials in advancing melanoma treatment.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











