1. The kidneys perform several important functions including regulating fluid balance, electrolyte and acid-base homeostasis, and producing hormones like renin and erythropoietin.
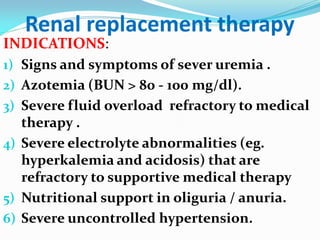
2. Acute renal failure in children results in impaired waste excretion, water and electrolyte dysregulation, and loss of acid-base control over hours to days.
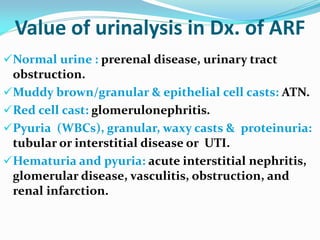
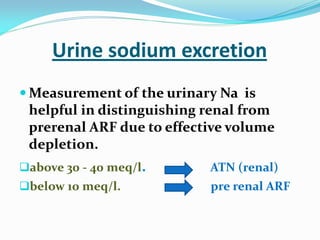
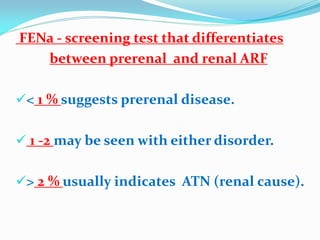
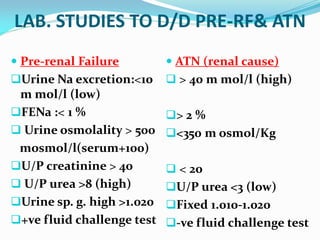
3. Causes include prerenal issues like dehydration, decreased blood pressure, or intrinsic renal problems such as glomerulonephritis, tubular injury, or nephrotoxins; evaluation involves lab tests, imaging, and assessing response to fluid resuscitation.




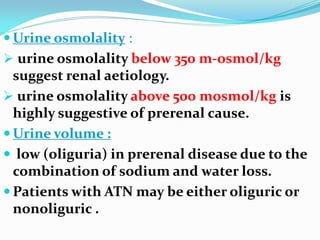
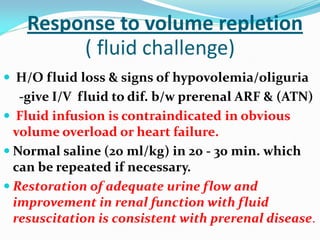
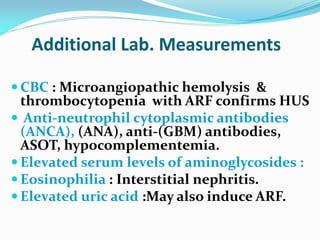
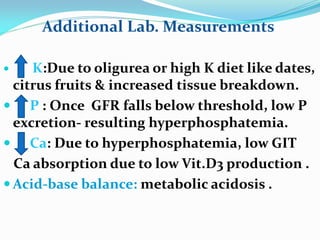
![Oliguria and fluid management[1]](https://cdn.slidesharecdn.com/ss_thumbnails/oliguriaandfluidmanagement1-110314134337-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


