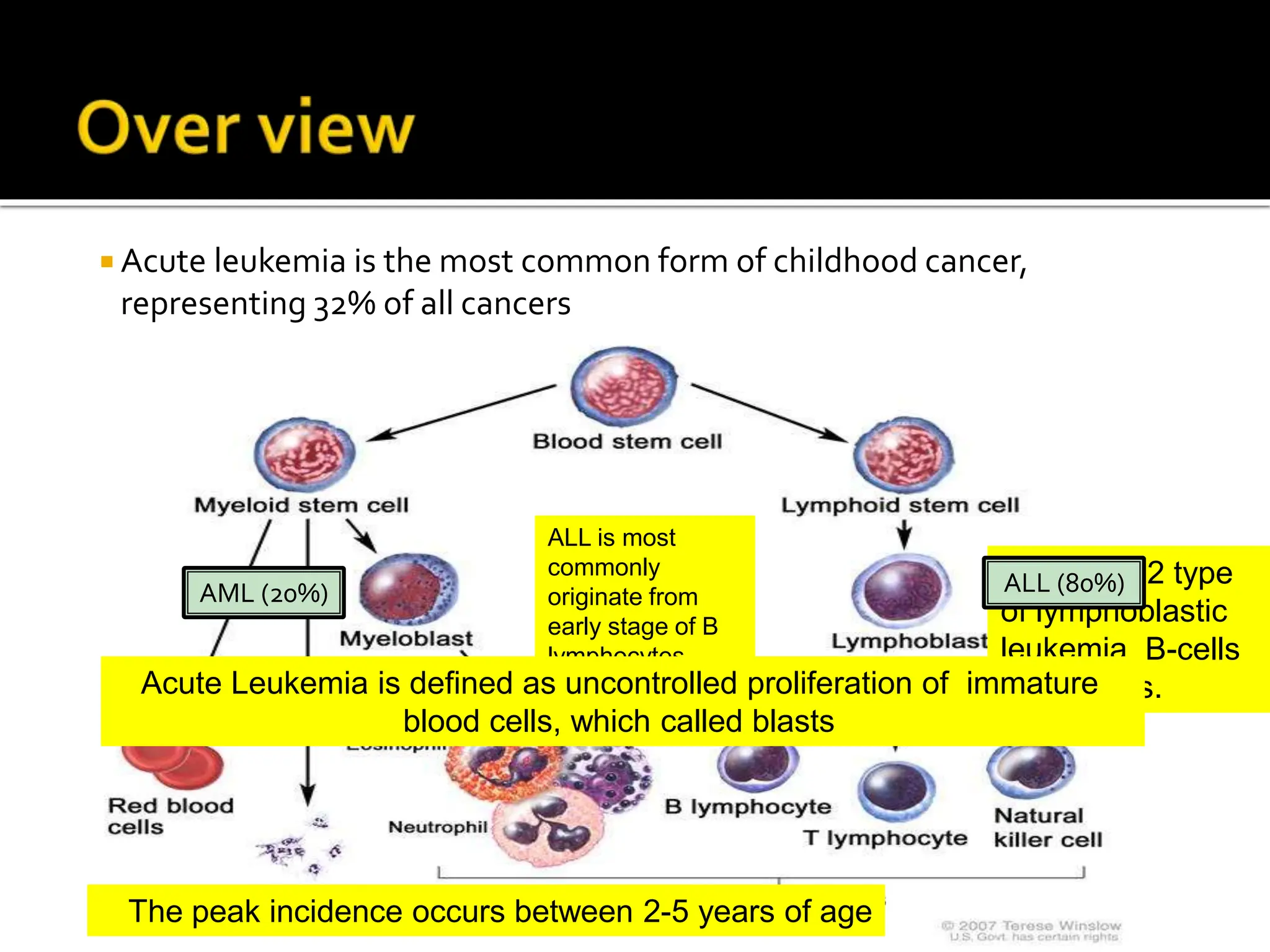
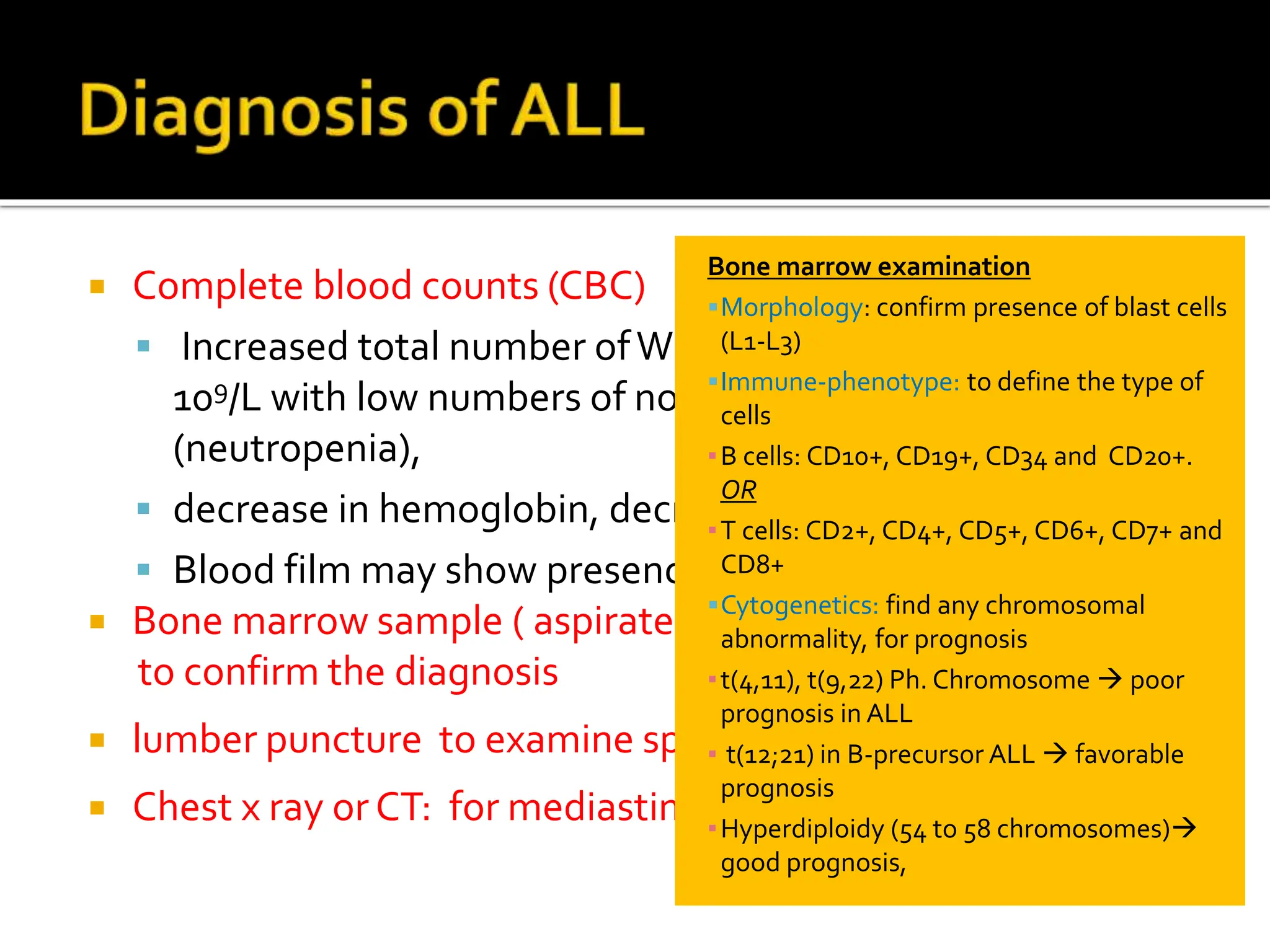
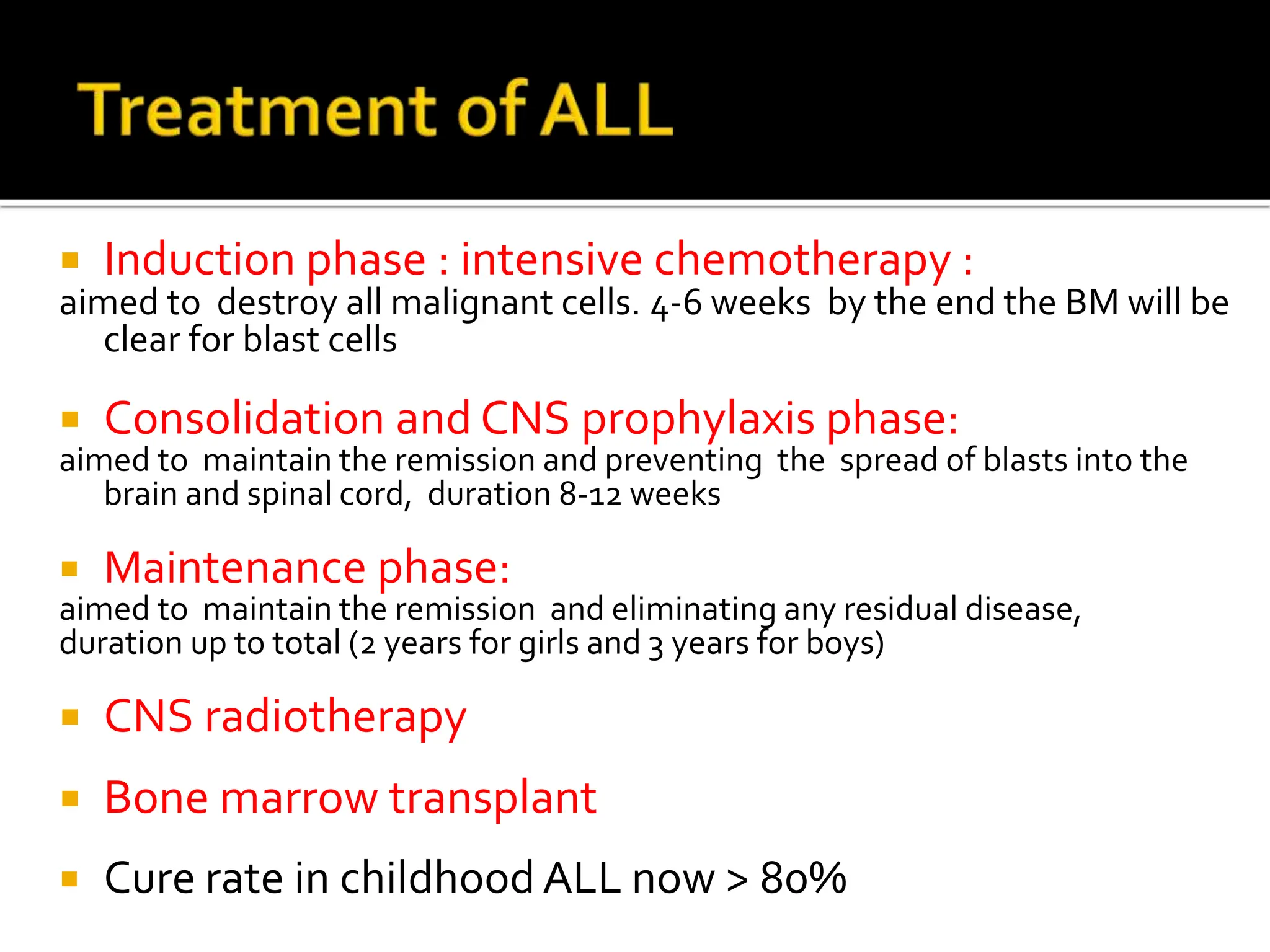
This document provides an overview of acute lymphoblastic leukemia (ALL) in children. It discusses the case of a 2.5 year old boy named Mohammad who presented with weakness, bone pain, and fever. His examination showed pallor, bruises, and an enlarged spleen. Laboratory tests confirmed B-lineage ALL. The standard treatment for ALL involves intensive chemotherapy divided into induction, consolidation, and maintenance phases lasting 2-3 years total. The goal is to destroy all cancer cells and prevent recurrence. With current therapies, the cure rate for childhood ALL is now over 80%.