Downloaded 63 times


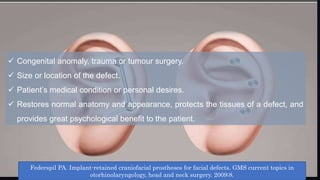
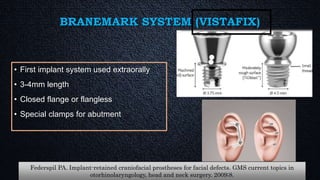
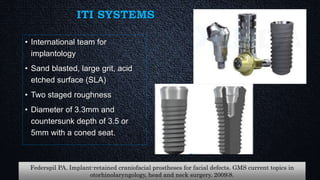
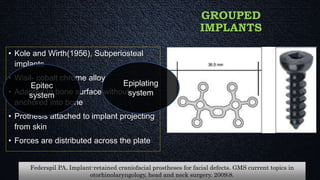
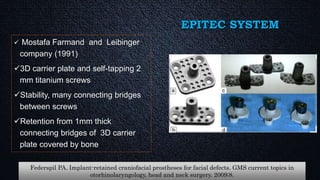
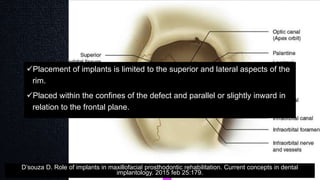
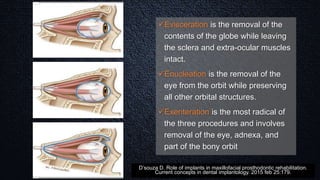
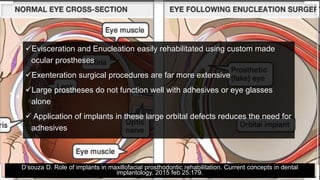
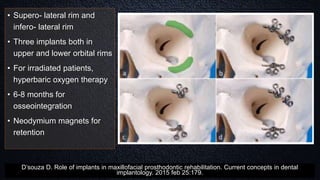










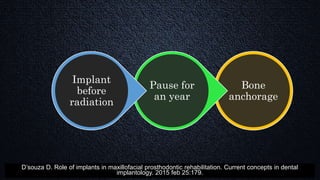
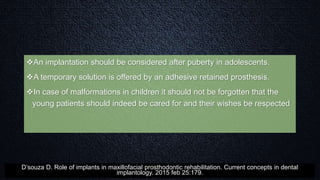

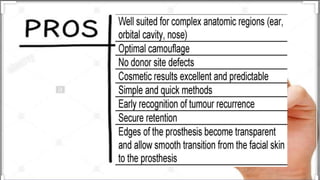
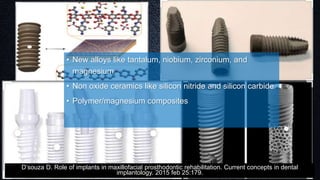
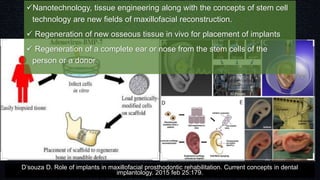


The document discusses implant-retained maxillofacial prostheses, highlighting their historical evolution, biomechanical and prosthetic considerations, and scopes of application such as auricular, orbital, and nasal prostheses. It covers surgical techniques, advantages of bone anchorage, and specific implant systems used in maxillofacial rehabilitation. Additionally, it addresses the psychological benefits and restoration of function and aesthetics for patients with facial defects due to congenital anomalies, trauma, or tumors.















![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)



















































