UNIT-4
Reproductive biology andsafe motherhood Programme
Safe abortion and CAC , PAC services
Supervised by
Respected ma’am
Rambha Sigdel
Assosiate Professor
Department of CHN
Presented by
Krista Rajbanshi
2.
• Key facts
•Definition
•History
•Abortionlaw in Nepal
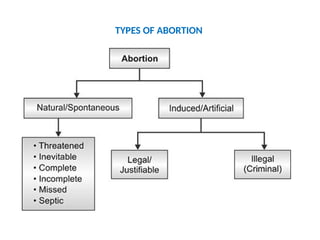
•Types
•Etiology
•Method of termination
•MVA
• Medical termination
• Complication
• Comphrensive abortion care
• Post abortion care
3.
KEY FACTS (WHO,2024)(1/3)
•Six out of 10 unintended pregnancies end in
induced abortion.
• Abortion is a common health intervention.
4.
KEY FACTS (WHO,2024)(2/3)
•It is very safe when carried out using a method
recommended by WHO, appropriate to the
pregnancy duration and by someone with the
necessary skills.
• However, around 45% of abortions are unsafe.
5.
KEY FACTS (WHO,2024)(3/3)
•Unsafe abortion is an important preventable cause of
maternal deaths and morbidities.
• It can lead to physical and mental health complications
and social and financial burdens for women,
communities and health systems.
• Lack of access to safe, timely, affordable and respectful
abortion care is a critical public health and human
rights issue.
6.
INTRODUCTION(1/2)
• Abortion isthe expulsion or extraction from its
mother of an embryo or fetus weighing 500
gm or less when it is not capable of
independent survival (WHO).
7.
INTRODUCTION(2/2)
• This 500gm of fetal development is attained
approximately at 22 weeks of gestation. The
expelled embryo or fetus is called abortus. The
term miscarriage which, is mostly used, is
synonymous with spontaneous abortion.
8.
Definition (1/3)
• Medico-legal definition: Abortion is the
termination of pregnancy before the period of
viability which is considered to occur at 20
weeks.
9.
Definition (2/3)
Safe abortion- Safe abortion is a medical
intervention to terminate the pregnancy by
skilled trained health care professional in a well-
equipped environment meeting all the minimal
medical standards.
10.
Definition (3/3)
Unsafe abortion– According
to WHO, Unsafe abortion is “a
procedure for terminating an
unwanted pregnancy either by
persons lacking the necessary
skills or in an environment
lacking the minimal medical
standards, or both.”
11.
INCIDENCE OF ABORTION
•Around 73 million induced abortions take
place worldwide each year. Six out of 10 (61%)
of all unintended pregnancies, and 3 out of 10
(29%) of all pregnancies, end in induced
abortion.
• Around 45% of all abortions are unsafe, of
which 97% take place in developing countries.
(25 November 2021-WHO)
12.
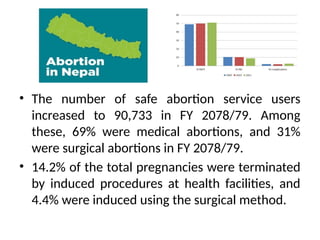
• The numberof safe abortion service users
increased to 90,733 in FY 2078/79. Among
these, 69% were medical abortions, and 31%
were surgical abortions in FY 2078/79.
• 14.2% of the total pregnancies were terminated
by induced procedures at health facilities, and
4.4% were induced using the surgical method.
13.
• Ancient Period:Abortion was viewed as a sin rooted in
religion, customs, and traditions.
Manusmriti: Considered abortion spiritually impure.
Kirant Era: Viewed as immoral, but lacked legal trial systems.
Lichhchhavi Era: No specific laws, but moral punishment
existed.
Malla Era: Laws were made more liberal to protect high-
caste interests; abortion allowed in caste-mixed pregnancies.
14.
• Shah Era(1910 BS): The Muluki Ain had the first formal
legal provision on abortion, penalizing both the woman
and the abortion provider with imprisonment or a fine.
• Before 2002 (2059 BS): Abortion was illegal and
criminalized, resulting in imprisonment, especially of
women. Unsafe abortions led to up to 50% of maternal
deaths and 60% of hospital admissions for complications
15.
• 2002: Abortionwas decriminalized, allowing
women legal access to services.
• 2004: Government abortion services began
at Maternity Hospital, Kathmandu.
• 2009: Medical abortion was introduced and
later scaled nationwide.
16.
Since 2017: Freeabortion services available at public
hospitals.
By 2021:
• 4,500 clinicians trained to provide safe abortion services.
• Different providers allowed abortions based on
gestational limits (e.g., ANMs up to 10 weeks, MBBS up
to 12 weeks, Ob-Gyns up to 28 weeks).
• 1,516 facilities accredited for safe abortion; 34 hospitals
approved for second-trimester procedures.
17.
Current System
Federal, provincial,and local governments manage
supplies, training, and medication.
Public-sector facilities receive reimbursement:
• NPR 800 (up to 12 weeks)
• NPR 2,000 (13–28 weeks)
• NPR 3,000 (for complication management)
ETIOLOGY(1/6)
Fetal causes
• Diseasedor maldeveloped or defects in
fertilized ovum
• Chromosomal abnormalities: trisomy,
balanced translocation
• Blighted ovum
20.
ETIOLOGY(2/6)
• Hydropic degenerationof villi, hydatidiform
mole
• Multiple congenital defects
• Multiple pregnancies
• Maternal causes (General and local
21.
ETIOLOGY(3/6)
Maternal causes (Generaland local)
General factors
• Endocrine imbalance any deficiency of estrogen
and progesterone
• Acute infection: toxin, malaria, influenza, syphilis
• Maternal disease such as chronic nephritis,
diabetes mellitus, hypertension, hypo and
hyperthyroidism, ABO/RH incompatibility
22.
ETIOLOGY(4/6)
• Diet deficitin proteins and vitamins
• Severe hypoxia: shock from hemorrhage
• Surgery and trauma e.g. direct trauma,
amniocentesis
• Severe mental stress including emotional
neurogenic shocks.
23.
ETIOLOGY(5/6)
Local factors
• Placentaprevia
• Uterine developmental anomalies: bicornuated uterus,
arcuate uterus, subsepted uterus etc.
• Fibroid uterus
• Incompetent cervix especially due to past birth trauma
• Surgery during pregnancy especially, myomectomy,
appendix or cyst removal in the first trimester
• Local trauma
24.
ETIOLOGY(6/6)
Fraternal cause
• Defectivesperm
• Men working in lead, mercury, x-ray etc
• Excessive consumption of alcohol and
cigarette smoking
• Men suffering from syphilis and tuberculosis
25.
METHODS OF TERMINATION
Firsttrimester (up to 12 weeks)
• Menstrual regulation (MR): MR
is the aspiration of the
endometrial cavity with 14 days
of the missed period in a
previously normal cycle when the
presence of an early pregnancy
cannot be diagnosed accurately
27.
Second Trimester
• Intrauterineinstillation of
hypertonic solution
• Prostaglandins. F2a or E2
and their analogues
• Oxytocin infusion
• Hysterectomy
28.
Immediate
• Trauma tothe cervix and uterus
leading to hemorrhage and
shock.
• Thrombosis or embolism
• Shocks and severe bleeding due
to incomplete abortion, atonic
uterus or rarely coagulation
failure.
29.
Remote
• Gynecological
• Menstrualdisturbance
• Chronic pelvic inflammation
• Infertility due to cornual block
• Scar endometriosis (1%)
30.
Obstetrical
• Recurrent abortiondue to cervical
incompetence
• Ectopic pregnancy
• Premature labor
• Dysmaturity
• Increased perinatal loss
• Rupture uterus
• Rh Iso-immunization in Rh negative women
if injection anti D immunoglobulin not given.
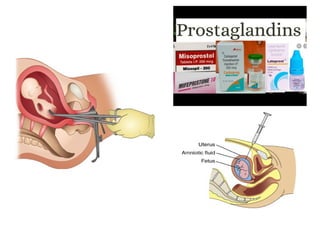
Medical termination
Regimen
• Therecommended regimen for pregnancies
up to 10 weeks is:
• Mifepristone 200 mg orally (swallowed)
followed by,
• Misoprostol 800 mcg sublingually (under the
tongue) or intra-vaginal 24 hours after
mifepristone
34.
Mannual Vaccum Aspiration
(1/4)
MVAis an effective method (procedure), for
treatment of incomplete abortion by removing
the contents of uterus with suction. MVA is a
method by which the contents of the uterus
are evacuated through a plastic or metal
cannula that is attached to a vacuum source
35.
Mannual Vaccum Aspiration(2/4)
Criteria for MVA
• Uterine size less than or equal to 12 weeks.
• Woman’s condition should be stable.
• Pulse less than 110/min.
• B.P. more than 60 Diastolic.
• Hb equal or more than 7 gm%.
• Per vaginal bleeding less than few days.
• Os should be opened
36.
Mannual Vaccum Aspiration(3/4)
Indication for MVA
• Non-viable intrauterine pregnancy, other
spontaneous abortion in progress.
• Undesired pregnancy of 12 weeks gestation or
less.
• No clinical evidence of active uterine or
cervical infection.
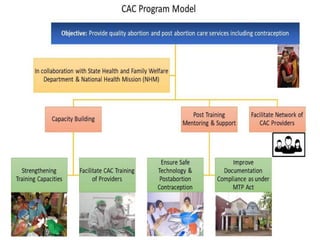
COMPREHENSIVE ABORTION CARE(CAC)
Introduction(1/ 3)
• Comprehensive Abortion Care (CAC)
is an approach of providing abortion
care services that address various
factors of the woman’s health needs
physical, mental, her personal
circumstances as well as her ability to
access the service
40.
Introduction(2/ 3)
• ComprehensiveAbortion Care (CAC) includes
affordable, acceptable, equitable, accessible
and quality of abortion care & other
reproductive health service
• e.g., counselling & informed consent for the
termination of pregnancy
41.
Introduction(3/ 3)
• informedchoice for the post abortion family
planning, identification & treatment of
sexually transmitted infections / reproductive
tract infections.
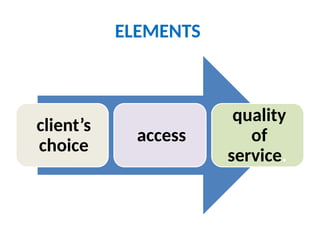
Client’s choice includes
•Right to choose the options ,abortion
methods, informed consent ,accurate and
complete information.
45.
Access
• The clientmust have access to service
providers, site and abortion care in every level
of country.
46.
Quality of service
•Ensuring confidentiality, privacy, respect &
positive interaction between women & health
facility staff.
49.
Introduction (1/2)
• Postabortion Care PAC is an important
intervention to address complications related
to spontaneous and induced abortions by
improving treatment and linking clients to
contraceptive care and other reproductive
health services.
50.
Introduction (2/2)
• PACis a package of integrated services
provided to clients who have had
miscarriages, induced abortions, or are
experiencing abortion-related complications
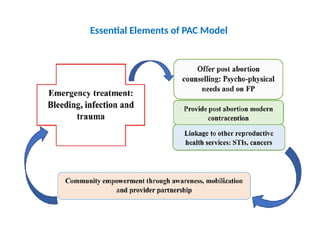
Elements of postabortion care
• Counselling & client provider interaction.
• Quality of service provided (treatment of
incomplete & unsafe abortion & complication).
• Post abortion contraceptive & FP services.
• Reproductive & other health service.
• Community & service provider partnerships &
mobilization of community resources.
• Prevention of unwanted pregnancy & unsafe
abortion.
53.
Considerations for post-abortioncare
• Eligibility criteria: Open cervical os, vaginal
bleeding or a history of vaginal bleeding
during the pregnancy & uterine size also
considered.
54.
• Uterine sizemay be smaller than the woman’s
report of her gestational age because some of
the uterine contents have already been
expelled.
• A woman’s eligibility for uterine evacuation
method for PAC should be guided by uterine
size rather than LMP.
55.
Management of shock
Managehemorrhage
Management of sepsis
Management of Genital Tract Trauma
Management of Intra-Abdominal
Injury
Pain management
58.
REFERENCES
• Marshall, J& raynor, M.Myles textbook for midwives.17th
edi. (2014).churchill
Livingstone.
• Dutta, DC.textbook of obstetrics .9th edi.new central book agency.pvt.ltd.150-165.
• Tuitui R,Suwal SN,Mannual of midwifery I, Vidyarthi pustak bhandar. 11thedition,
2016.215-250
• Wikipedia.Abortion November 19.https://en.wikipedia.org/wiki/Abortion_in_Nepal.Puri
M, Singh S, Sundaram A, Hussain R, Tamang A, Crowell M. Abortion Incidence and
Unintended Pregnancy in Nepal. Int Perspect Sex Reproductive Health. 2016 Dec.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5568822/
• Essential Elements of Post abortion Care. Retrieved [29 may2025]: Available from
https://www.guttmacher.org/journals/ipsrh/2003/09/essentia l-elements-postabortion-
care-origins-evolution-and-futuredirections
• Post abortion care. Retrieved [29 may 2025]: Available from
https://www.globalhealthlearning.org/sites/default/files/refer encefiles/Essential
%20Elements%20of%20Postabortion% 20Care.pdf





![REFERENCES
• Marshall, J & raynor, M.Myles textbook for midwives.17th
edi. (2014).churchill
Livingstone.
• Dutta, DC.textbook of obstetrics .9th edi.new central book agency.pvt.ltd.150-165.
• Tuitui R,Suwal SN,Mannual of midwifery I, Vidyarthi pustak bhandar. 11thedition,
2016.215-250
• Wikipedia.Abortion November 19.https://en.wikipedia.org/wiki/Abortion_in_Nepal.Puri
M, Singh S, Sundaram A, Hussain R, Tamang A, Crowell M. Abortion Incidence and
Unintended Pregnancy in Nepal. Int Perspect Sex Reproductive Health. 2016 Dec.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5568822/
• Essential Elements of Post abortion Care. Retrieved [29 may2025]: Available from
https://www.guttmacher.org/journals/ipsrh/2003/09/essentia l-elements-postabortion-
care-origins-evolution-and-futuredirections
• Post abortion care. Retrieved [29 may 2025]: Available from
https://www.globalhealthlearning.org/sites/default/files/refer encefiles/Essential
%20Elements%20of%20Postabortion% 20Care.pdf](https://image.slidesharecdn.com/unit4abortion-250802150328-15707248/85/ABORTION-CAC-PAC-SERVICES-IN-WORKD-AND-NEPAL-58-320.jpg)


![Understanding abortion and Concept of CAC (2) [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/understandingabortionandconceptofcac2autosaved-260130124423-bbc9b8d3-thumbnail.jpg?width=640&height=640&fit=bounds)





















































