GENERAL OBJECTIVES
• Atthe end of the presentation,
students should demonstrate an
understanding on the different types of
abortion and be able to offer
comprehensive care to prevent
complications.
3
4.
SPECIFIC OBJECTIVES
At theend of the lesson, students should
be able to;
•Define the terms (i). Abortion
(ii). Unsafe abortion.
•State the causes of Abortion.
•Outline the classification of Abortions.
•State the signs and symptoms of
abortion.
5.
SPECIFIC OBJECTIVES
cont’d…
• Describepost abortal care.
• Discuss the specific management of
different types of abortion.
• List the complications of abortions.
• Mention the standard guideline for
termination of pregnancy.
6.
INTRODUCTION
• According toreports, incidence of
abortions has declined worldwide due
to access to family planning education
and contraception. Up to 15% of all
pregnancies and approximately 30% of
all first pregnancies end in
spontaneous abortion.
6
7.
INTRODUCTION cont’d..
• Atleast 75% of miscarriages occur
during the first trimester. Further, about
42 million abortions are estimated to take
place annually worldwide with 22 million
occurring safely and 20 million unsafe
and result in about 70 000 deaths .
Complications of unsafe abortions are
said to account for 13% of all maternal
deaths globally (PRB, 2011).
7
8.
INTRODUCTION
cont’d..
• In Zambia,it is estimated that up to
30% of maternal deaths are due to
unsafe abortion. About 23% of
incomplete abortions occur among
women younger than 20 years, 25%
maternal deaths due to induced
abortions were in girls younger than 18
yrs.
8
9.
INTRODUCTION
cont’d
• 30-50% ofacute gynaecological
admissions are currently as a result of
abortion complications (MoH, 2009).
Therefore, addressing abortion in
reproductive health is key to attaining
the 5th millennium development goal
that aims to reduce maternal mortality
by three quarters by 2015.
9
10.
DEFINITION OF ABORTION
•Abortion - is defined as the
termination of pregnancy by the
removal or expulsion of a fetus or
embryo prior to viability or before 28th
week of gestation from the uterus of in
Zambia (MOH, 2001).
10
11.
Unsafe Abortion
• WorldHealth Organization (WHO,
2008) defines Unsafe Abortion as “a
procedure for terminating an
unintended pregnancy that is carried
out either by persons lacking
necessary skills or in an
environment that does not conform
to minimal medical standards, or
both”.
11
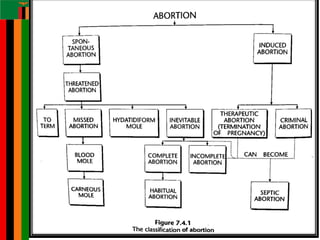
12.
CAUSES OF SPONTANEOUS
•The cause is Idiopathic (majority) –
cause unknown
• Associated factors include:
1. Fetal causes
2. Maternal cases
3. Risk factors
4. Environmental factors
12
13.
Fetal causes
• Geneticabnormalities - Chromosomal
anomalies or replication defect
accounts for 50% of abortion cases.
• Abnormal placenta
13
14.
Maternal causes
• Endocrineabnormalities – Poor
development of the corpus luteum,
inadequate secretory endothelium and
low serum progesterone levels lead to
failure of the pregnancy to be
maintained.
14
15.
Maternal causes cont’d…
•Maternal infections – Diseases
acquired during pregnancy such as
rubella, febrile conditions like
malaria,Toxoplasmosis,
cytomegalovirus, syphilis, Chlamydia
and malaria are the common infections
that can cause abortion.
15
16.
Maternal causes cont’d
•Anatomic uterine defects: -
Retroversion of the uterus, bicornuate
uterus, unicornuate uterus and fibroids
hinder the growth of the fetus.
16
17.
Maternal causes cont’d
•Medical disorders –
conditions such as anaemia,
hypertension, renal diseases, and
cardiac diseases lead to placental
insufficiency. Poor placental perfusion
makes it weaker and eventually starts
detaching causing abortion
17
18.
Risk Factors
1. Age
Riskincrease with age because of
degeneration of the ovaries which leads
to low levels of progesterone which
maintains the pregnancy.
•Age of 20 – 30 years risk ranges from 9
– 17%. 40 years 40% and 45 years
80%. Risk
increases as age increases.
18
19.
Risk Factors cont’d...
2.Trauma – e.g. when doing chorionic
villus sampling, amniocentesis).
3. Incompetent cervix;
•Recurrent premature dilatation of the
cervix i.e. previous induced abortions
and congenital cervical defects are the
main causes of cervical incompetence.
19
20.
3. Stress andanxiety this is due to the
effects of stress hormones which cause
vasoconstriction leading to reduced
blood supply to the fetus.
20
21.
Environmental/ social factors
•Caffeine from coffee, nicotine from
cigarette smoke cause vasoconstriction
leading to poor placental and fetal
perfusion causing abortion.
• Alcohol consumption leads to maternal
malnutrition.
• Exposure to organic solvents such as
lead
21
Signs and symptoms
ThreatenedAbortion
•Amenorrhea followed by slight Per
Vaginal Bleeding (PVB) which may be
Intermittent or continuous bleeding
•May or may not be accompanied by mild
cramping and back pain
•Uterine size correct to gestational dates
•Cervix is closed
24
25.
Signs and symptomscont’d..
• Inevitable Abortion
• Amenorrhea followed by heavy vaginal
bleeding
• Progressive dilatation of the cervix
• Abdominal pain is more severe, colicky
in nature and located in the supra
pubic area
25
26.
Signs and symptomscont’d..
• Amniotic membranes may be felt
bulging into the cervical canal or may
be already ruptured and fetal parts
palpable
• May be complete or incomplete
26
27.
Signs and symptomscont’d..
Complete abortion
•The term “complete abortion” signifies
that all products of conception have
been expelled.
•Uterus becomes smaller on palpation
•On vaginal examination cervix is closed
27
28.
Signs and symptomscont’d..
• Patient usually notices expulsion of the
tissue or even fetus and placenta
• Abdominal pain subsides
• Bleeding may stop or slows down
considerably
28
29.
Signs and symptomscont’d..
• Incomplete abortion
• Expulsion of products of conception is
incomplete
• Abdominal pain continues although
may be less severe
• Bleeding continues and becomes
heavier!?
29
30.
Signs and symptomscont’d..
• Uterus enlarged, palpable and may
feel boggy
• Cervix may either be dilated or closed,
but will feel patulous
• Signs of shock if severe bleeding
30
31.
Signs and symptomscont’d..
• Placenta and fetus may appear to
have been expelled intact, but some
trophoblastic or placental tissue
remain adhering to the uterine wall
causing profuse bleeding
• Products of conception may be felt or
seen
31
32.
Signs and symptomscont’d..
Missed abortion
•Features;
• This may or may not be heralded by
vaginal bleeding or abdominal pain
•Vaginal bleeding stops and patient
continues to be amenorrheic
•In some other cases vaginal bleeding
continues intermittently and usually is dark
brown discharge
33.
Signs and symptomscont’d..
• Fetal movements if felt before, ceases
• Symptoms of early pregnancy begin
to disappear
• Uterine size remain stationery or even
decreases
• Cervix is closed
• Fetal heart cannot be heard by either
fetoscope or Doppler
33
34.
Signs and symptomscont’d..
• Pregnancy test usually is negative
• process of abortion will eventually start
spontaneously 4-5 weeks
• The main complication of missed
abortion is development of
Disseminated Intravascular
Coagulation (DIC)
34
35.
Signs and symptomscont’d..
Septic abortion
•Per vaginal bleeding with pain
•Amount of bleeding is variable and pain is
suprapubic constant and severe
•Patient feels weak and complains of
headache, malaise and seem to be
extremely ill
•Chills and fever signifies serious infection
35
36.
Signs and symptomscont’d..
• Most serious complications of septic
abortion is septic shock characterized
by hypotension with tachycardia,
normal or subnormal temperature
• Generalized abdominal tenderness
with rebound tenderness, rigidity or
distension are signs of spreading
peritonitis
36
37.
Signs and symptomscont’d..
• On vaginal examination cervix is open
with foul smelling purulent bloody
vaginal discharge
• Products of conception may be felt in
cervical canal or inside the uterine
cavity
• Cervical motion elicits severe
tenderness
37
38.
POST ABORTAL CARE
(PAC)
Postabortal care is a Series of medical
and related interventions designed to
manage the complications of
spontaneous and induced abortion (both
safe and unsafe) and address women’s
related health care needs.
38
39.
PAC cont’d..
PAC isa global initiative to reduce
maternal morbidity and mortality and to
improve women’s sexual and
reproductive health and lives. It is a
Model of care that consists of five
elements;
39
40.
Essential Elements ofPAC
• Community and provider partnerships
• Counseling - to respond to women’s
needs
• Treatment of incomplete and unsafe
abortion.
• Contraceptive and family planning
services.
• Reproductive and other services
40
41.
Advantages of PAC
•Can be included in the existing range of
services or as a separate, vertical service
• Is acceptable where induced abortion is
legally restricted
• Links curative service (treatment for
complications) with preventive service (i.e.
family planning).
• Can be offered successfully in low resource
settings
41
42.
Information, Education and
Communication(IEC)
• During IEC, Involve the support person and
commence from the known to the unknown
• Hygiene/Prevention of infection
• Nutrition
• Rest
• Family planning
• Sexual advice
• Review date
42
43.
Comprehensive Abortion
Care
• Thisis an approach to abortion care
based on the epidemiological concept
of primary (prevention of pregnancy),
secondary (treatment of unwanted
pregnancy) and tertiary (treatment of
complications) in health care (MoH,
2009).
43
44.
Management of threatened
abortion
Incase of threatened abortion, care is
directed towards preservation of the
pregnancy. Bed rest is instituted though
there is lack of evidence to suggest this
as effective in preventing miscarriage.
44
45.
Management of threaned
abortioncont’d..
• The woman can be taken for an ultra
sound to confirm continuation of the
pregnancy. After bleeding has
diminished the cervix should be
examined to rule out dilatation. In a
few cases symptoms disappear and
the rest of the pregnancy is normal.
46.
Management of Inevitable
abortion
•Ultra sound shows no foetal heart beat
and the pregnancy test may still be
positive as Hcg is produced by the
chorion and not the placenta. With
time, the uterus expels the products of
conception.
46
47.
Management of Inevitableabortion
cont’d..
Treatment
•Admit the patient to a gynaecology
ward.
•Take urine sample for pregnancy test.
•Check the baseline observations of vital
signs.
•Blood can be taken to confirm rhesus
factor if not done
48.
Management of Inevitableabortion
cont’d..
• Medical assessment can be carried out
within 1 hour of arrival
• Ultra sound is done to detect retained
products and confirm diagnosis.
• Vaginal examination is done and will reveal
a dilated cervix with protruding products of
conception through the os.
• Oxytocin 20 units intravenously may be
given and oxytocin 10 iu i.m may be given.
48
49.
Management of Inevitableabortion
cont’d..
• The presence of positive pregnancy test,
pain, distress and heavy bleeding would
normally indicate the need for surgical
currretage.
• Adequate analgesia should be given to
relieve pain.
• Care of the patient who has had an
Inevitable abortion includes emotional
support and counselling during the grieving
process.
49
50.
Management of Inevitableabortion
cont’d..
• Privacy and dignity of the woman
should be maintained through out.
• Keep the support person informed of
what is happening.
• Rapidly assess the baby when it is
born depending on gestation and place
of birth to determine whether it can
live.
50
51.
Management of Inevitable
abortioncont’d..
• Inform the parents about the condition
and obtain assistance from a
paediatrician. Immediate transfer the
baby to a neonatal intensive care.
• If the baby dies, death should be
registered.
51
52.
Management of Inevitableabortion
cont’d..
• Encourage the woman and her partner
to express their feelings. Some
couples may want to talk to a member
of the clergy or, depending on their
religion, may wish to have the foetus
baptized.
52
53.
Management of Incompleteabortion
• Bleeding continues because part of
the placenta may adhere to the uterine
wall. Haemorrhage occurs because
the uterus does not contract and seal
the large vessels that fed the placenta.
53
54.
Management of Incompleteabortion
cont’d..
• Treatment
• Explain the procedure to the woman
and support person to alley anxiety.
• IV or intramuscularly oxytocin should
be given to control bleeding.
• Evacuation of retained products of
conception is done using manual
vacuum aspiration.
56.
Management of Incompleteabortion
cont’d..
• Before vacuum aspiration normal
saline is given to treat hypovoleamia.
• Maintain privacy during vacuum
aspiration.
• Give analgesia before vacuum
aspiration.
56
57.
Management of Complete
abortion
Uteruspasses all the products of
conception pain stops and signs of
pregnancy regress. The uterus is firmly
contracted on palpation and an empty
cavity is seen on ultra sound examination.
Minimal bleeding usually accompanies
complete abortion because the uterus
contracts and compresses maternal blood
vessels that fed the placenta.
57
58.
Treatment
• No furthermedical intervention is
needed except support following
pregnancy loss.
• Counselling and reassurance is given.
• The woman is advised to seek medical
advise if bleeding recurs or she
experiences pyrexia
58
59.
Management of Missed
abortion
•Uterus retains the products of
conception for 2 months or more after
the death of the foetus. The normal
reaction of the uterus to the death of
the foetus is to expel it but, for some
unexplained reason this may not occur
59
60.
• Absence offoetal heart pulsation is
detected by ultra sound. Uterine
growth ceases; uterine size may even
seem to decrease. Prolonged retention
of the dead products of conception
may cause coagulation defects, such
as disseminated intra vascular
coagulation.
60
61.
Treatment
• Prostaglandins maybe administered
or evacuation is done
• During evacuation, the cervix is gently
dilated to allow a small currete to be
introduced in the uterine cavity to
remove any retained products of
conception.
61
62.
Treatment cont’d..
• Prostaglandinsinserted vaginally
make the cervix favourable prior to
surgery.
• This avoids trauma to the cervix
caused by possible dilatation and
reduces the risk of cervical
incompetence in subsequent
pregnancies.
62
63.
Treatment cont’d..
• Bloodfor X-match, HB, grouping,
clotting time is taken in case of
hypofibrogenemia
63
64.
Management of Habitual
abortion
•This is spontaneous loss of three or more
consecutive pregnancies constitutes habitual
abortion.
• Treatment
• Depends on the cause for example if it is an
incompetent cervix, a shirodker suture can be
inserted, and if it is due to STIs treatment can
be given.
• Investigations can be done to establish the
cause.
64
65.
Management of Septic
abortion
•Infection accompanies this type of
abortion. This may occur with
spontaneous abortion but usually
results from an illegal or unsafe
abortion.
• Blood culture and vaginal swabs
should be taken to identify cause of
the infection.
65
66.
• IV antibioticsmaybe administered,
starting with broad spectrum and one
effective against anaerobic infections.
For example IV X-pen 2MU QID for 7
days and IV Flagyl 500mg TDS for 7
days.
66
67.
• Vacuum aspirationis done to remove
retained products of conception if they
are there. However there is high risk of
perforating the uterus in septic
abortion because it becomes friable.
• In a few instances, hysterectomy
maybe done
67
68.
Management of Induced
Abortion
•There are two main forms of inducing
a therapeutic abortion, Medical and
surgical.
• Medical abortion
• The abortion pill -This involves taking
medicines to end the pregnancy.
68
69.
• Mifepristone istaken orally and works
by blocking the hormone
progesterone. Without progesterone
the endometrium breaks down and the
pregnancy cannot continue.
• Misoprostol
69
70.
• For induction-Misoprostol tablet is
inserted into the vagina either by the
woman herself or by the healthcare
professional and it initiates uterine
contractions and cervical dilatation.
• Dose of Misoprostol For treatment
following abortion;
70
• Routes ofAdministration
• 600 mcg Oral - Three 200mcg pills
should be swallowed together with water.
• 400 mcg Sublingual. Sub lingual Hold the
pills under tongue until they dissolve , Any
remaining pill fragments can be
swallowed with water if they have not
already dissolved within 30 minutes
72
73.
• A lowerdose (400 mcg vs. 600mcg)
may be advantageous in settings
where the cost of misoprostol is high
73
74.
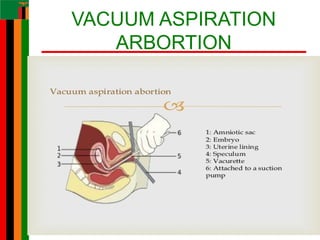
Surgical abortion:
• Thereare two types of surgical
abortion:
• Manual Vacuum aspiration (MVA)
• MVA is performed in pregnancies
below 15 weeks of gestation. Vacuum
aspiration uses gentle suction to
remove the pregnancy and takes
about 5-10 minutes from start to finish.
74
• It canbe done under local (cervical block) or
general anaesthesia. Patient is discharged
the same day after observing that the
general condition is good (WHO, 2012).
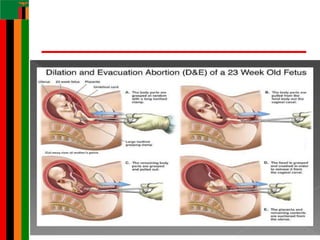
• Dilatation and Evacuation
• Usually performed between 15- 24 weeks of
pregnancy and under general anaesthesia
• (WHO, 2012)
77
• COMPLICATIONS OFABORTION
• Severe vaginal bleeding due to
retained products of conception
• Shock due to bleeding
• Secondary bacterial infections due to
use of unsterile instruments to abort or
from an endogenous infective
organism
• The Terminationof Pregnancy Act was
enacted in Zambia in 1972 and
amended in 1994. It is commonly
referred to as the TOP Act.
81
82.
• Women havethe right to know that
Safe Termination of pregnancy is legal
in Zambia and have the right to seek
more information and services from
qualified providers in their
communities. However, the law states
that safe termination of pregnancy is
available
82
83.
• when:
• Thereis risk to the life of the pregnant
woman.
• There is risk of injury to the pregnant
woman.
• The child will be born mentally or
physically handicapped.
•
83
84.
• When continuationof the pregnancy
puts the lives of other existing children
at risk.
• When the pregnancy is a result of rape
or defilement.
84
85.
Safe termination ofpregnancy
is legal in Zambia when:
• It is approved by 2 medical personnel.
• It is done in a clean, safe and
registered environment.
• It is done by a trained service provider.
• The woman makes a free, informed
choice without coercion has signed a
consent form.
85
86.
Amendment of theAct
• Amendment to the penal code was done in
2005 by the Zambian Parliament in
particular to sections that deals with gender
violence of female child; rape and
defilement; where a child is defiled or raped
and becomes pregnant, the pregnancy may
be terminated with accordance with the
Termination of Pregnancy act.
•
86
87.
CONCLUSSION
Abortion is oneof the causes of maternal
mortality as a result shock and septicaemia
if not well managed. All cases of abortion
should be considered incomplete until a
thorough investigation is done they should
therefore be treated as an emergency
because of the severe complications that
may arise if mismanaged such as maternal
death and severe bacterial infection.
88.
• Post abortalcare facilities must be
evenly distributed and Increased
material and skilled human resource
ensures quality care.
• Community sensitization on the
dangers of criminal abortions and
Family planning services will
tremendously reduce the impact of
unsafe abortion.
89.
• All stakeholdersto come on board so
that maternal morbidity and mortality
rates are reduced.
89
REFERENCES
• Fraser .M.Dand Cooper. M.A. (2003)
Myles Text book for midwives 14th
Edition Elsevier. Philadelphia
• Sellers M. P (2008). Midwifery A
Textbook and Reference Book for
Midwives in Southern Africa. Volume II
Juta and Co, Ltd, Lansdowne 7779.
91
92.
• WHO, (2012).Safe abortion:
technical and policy guidance for
health systems,
2n
editionwww.ippf.org/resource/IPPF-
Charter-Sexual-and-Reproductive-
Rights
92
#1 Speaker's Notes:
Abortion occurs commonly, yet it is stigmatized and hidden. This presentation describes the problems associated with unsafe abortion, and outlines strategies to address these problems.
I will begin by sharing information about abortion and unsafe abortion, and the international agreements that deal with this issue. Then, I will discuss how to offer safe abortion services—specifically focusing on clinical issues, how to organise services, and policy barriers. Recommendations here are based primarily on the World Health Organization’s 2003 publication: Safe Abortion: Technical and Policy Guidance for Health Systems.
Additional Resources:
You should feel free to customise the presentation, selecting modules or slides to best fit the purpose of the presentation and the interests of the audience. Some suggested versions of the slide presentation are available in the User’s Guide, which is included on this CD-ROM. The User’s Guide provides suggestions on which slides to select for health care providers, policymakers, advocates, and media.
This is also an appropriate time to inform your audience of rules for the presentation, such as whether questions should be asked at any time or saved until the end of the presentation.
#12 Genetic abnormalities - Chromosomal anomalies or replication defect accounts for 50% of abortion cases
#15 Bacteria, viruses and parasites invade the placenta and affect the metabolism of the placenta leading to early degeneration
#19 This is due to inadequate cervical collagen fibres which makes the cervical os weak leading to failure of the cervix to contain the weight of the growing fetus.
After 1st miscarriage, risk is 20%
After 3 miscarriages, risk is 43%.
#32 Refers to cases in which dead fetus or embryo has been retained in the uterus for more than 4-8weeks. After period of normal pregnancy the fetus dies
#34 Patient notices gum or nose bleeding or bleeding may occur after mild trauma (cutaneous ecchymoses)
#41 EVEV WHERE ONE HAS PERFORMED AN ELLIGAL ABORTION, THEY WILL STIL BE CARED FOR.