2
Outline
• Definition ofabortion
• Types of abortion
• Causes of abortion
• Managements of abortion
• Complications of abortion
• Comprehensive Post Abortion Care(cPAC)
3.
3
Definitions:
• Abortion: Terminationof pregnancy before
fetal viability.
• Before 28wks or 500gm(our setting), in
developed world before 20wks of Gestation.
• Incidence: about 10-20 % of all clinical
pregnancies ends in abortions.
4.
4
Types:
Spontaneous: Unintentional pregnancy
termination.
Induced:Intentional pregnancy termination.
• Induced abortion can be safe or unsafe
• Safe: Where the law permits, done by persons
with the necessary skills, in an environment
with acceptable medical standards, with less
complications.
5.
5
Cont:
• Unsafe: Donewhere the laws are restrictive, by
persons lacking the necessary skills, in an
environment lacking the minimal medical
standards, or both.
• It is associated with most complications, has high
rate of mortality and morbidity.
• Worldwide, annually - 20 million unsafe
abortions
- 80,000 deaths.
• It can be legal /Illegal
6.
6
AETIOLOGY
Chromosomal abnormalities; almost50% of first
trimester abortions, 70% of pregnancy loss
before 20 weeks. Examples: trisomies, partial
deletion,aneuloids etc.
Maternal anatomic anomalies — such as uterine
leiomyomas (fibroids), polyps, adhesions, or
septa, may be associated with pregnancy loss
based on their size and position in relation to the
developing pregnancy.
7.
05/05/2025 7
• Trauma— trauma that results in direct impact
to the uterus can cause pregnancy loss. This can
be due to violent trauma (gunshot wounds,
penetrating injuries) or iatrogenic trauma, as
with chorionic villus sampling and amniocentesis.
8.
05/05/2025 8
• Infection,including chorioamnionitis and maternal viral infection
• Chronic stressors, including contributions from racial/ethnic, financial or other
disparities, chronic food or housing insecurity, and other long-term life stressors
• Uterine malformation ie Asherman syndrome, Developmental Mullerian duct
abnormalities or fusion defects, in utero exposure to diethylstilbestrol.
• Cervical insufficiency
• Fetal malformation or syndromes such as anencephaly, trisomies, renal agenesis, or
hydrops
• Autoimmune disorders ie Thrombophilias, SLE, APS
• Pregnancy event ie Abruption, early PPROM, preterm labor
• Endocrine abnormalities: DM, Hyper and Hypothyroidism, progesterone deficiency.
• Environmental factors: Tobacco, caffeine, alcohol, radiation and IUCDs.
9.
9
Categories of SA
ThreatenedAbortion: Symptoms and signs coincide with its
duration.
• Vag. Bleeding, slight, bright red.
• LAP- absent or slight
• USS- live fetus
• Cervix os- not dilated.
Management: Restricted physical activities including intercourse
– Follow up seven days
– Counsel on danger signs
• Progesterone and gonadotrophins role is controversial.
10.
10
Inevitable abortion
• Symptomsand signs coincide with its duration
• ROM btn 12-28 wks may be a sign.
• Excessive Vaginal Bleeding, colicky LAP, radiating to the back
• Internal os is dilated
– Management: ABDC
– Manage pain
– Observe for spontenous expulsion for 6 hours
– Or Perform MVA if GA 12 weeks and below
– If above 12 weeks
• Augment with oxtocin
• Or give misoprostol
• If still there are product of expulsion manage as incomplete abortion
11.
11
Incomplete Abortion
• Partof the POC has been expelled
• Clinically: Some products have passed out, continuous
vaginal bleeding.
• Uterus is less than GA, Cervix is open, retained POC may be
felt through it.
1. Management: ABCD (resuscitation)
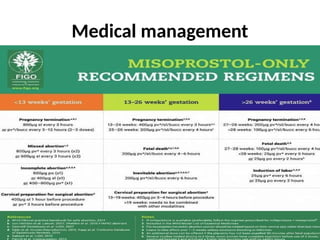
2. Medical
• Misoprostol (PGE1)
3. Surgical methods
Manual Vacuum Aspiration (MVA) (GA <12Weeks)
Dilatation and curettage (>12 weeks))
12.
12
Complete abortion
• AllPOC expelled out
• Clinically: no/minimal vaginal bleeding, less abd.
Pain
• Uterus slightly larger than normal, cervix closed.
• Management;
– Antibiotics
– Fefol
– Reassess after four weeks
13.
13
Missed abortion
• Retentionof dead POC for more than 4 wks.
• Carneous mole_ a dead ovum in early pregnancy,
surrounded by clotted blood.
• Clinical picture: May present with feature like
threatened abortion.
• Regression of pregnancy symptoms
• Abdomen doesn’t increase or even decrease
• May have milk secretion(increase prolactin
production.
14.
14
Cont:
• A darkbrown discharge may occur
• Signs: Uterus decreases, cervix closed/open
• UPT may become negative after 2 wks
• USS- a collapsed gestation sac, absent fetal
movements
• Complications: DIC and superadded infection
• Management: evacuation
15.
15
Cont:
• Evacuation: Lessthan 12 wks, suction
evacuation. More that 12 wks prostaglandins,
oxytocins or a combination of both
16.
16
Septic Abortion
• Anyabortion complicated by infection
• Clinical features: Pyrexia, tachycardia, rigors,
hypothermia, malaise, sweating, headache,
joint pains. Hematuria, jaundice is an ominous
sign.
• Abdominal Exam: Suprapubic tenderness,
abdominal distension and rigidity indicate
peritonitis.
17.
17
Cont:
• Local examination:Offensive discharge
• Minimal discharge is associated with severe
cases.
• Tender uterus, POC may be felt
• Fullness and tenderness of the POD indicate
pelvic abscess, which may cause diarrheal.
• Complications: Endotoxin shock, ARF, or DIC.
18.
18
Management of septicAbortion
• Resuscitation: IV Fluids and BT if indicated.
• Broad spectrum antibiotics. IV Ampicillin or
Cephalosporin + Gentamicin + Metronidazole
• Anti gas gangrene ( In C.welchii) anti tetanus
serum in ( C. tetani)
• Uterine evacuation: Uterotonics, MVA or D & C
• Endocervical swab for C & S
• Hysterectomy may be indicated.
19.
19
Complications of Abortion
•Contributes to 13-15% of Maternal mortality.
• Immediate : Haemorrhage, infection, injury to
internal organs, pelvic abscess, peritonitis
• Toxicity from abortifacients used.
• Long term: Infertility 2%, chronic pelvic pain
5% and increased risk of ectopic pregnancy
and premature delivery.
20.
Comprehensive Post Abortioncare(cPAC)
• A package of services as an approach of
managing patients with abortion or
abortion-related complications
• Main aim is to reduce mortality and
morbidity
• It increase contraception uptake
• Improving women's sexual and reproductive
health
21.
05/05/2025 21
Components ofcPAC
1. Treatment of incomplete, missed and septic abortion
2. Counseling to identify and respond to women’s emotional
and physical health needs
3. Contraceptive and family-planning services to help women
prevent future unwanted pregnancies and abortions
4. Reproductive and other health services that are preferably
provided on-site or via referrals to other accessible facilities
5. Community and service-provider partnerships to prevent
unwanted pregnancies and unsafe abortions, to mobilize
resources to ensure timely care for abortion complications,
and to make sure health services meet community
expectations and needs.
22.
1.Treatment
• Treatment ofincomplete and unsafe abortion
and complications that are potentially life
threatening is an important component of
PAC.
• In many cases, an incomplete abortion will
need to be treated by uterine evacuation.
• Complications may be potentially life
threatening if prompt and appropriate medical
attention is lacking.
23.
2. Counselling
• Effectivecounseling - permeate every component of
services, from 1st contact between the woman and
provider to the last contact.
• Women and service providers - identify and address
broader emotional and physical health and other
needs and concerns.
• Providers should be able to respond or provide
referrals within their service network.
24.
3. Contraceptive+Family planningservices
• Many women of childbearing age would want to
delay/avoid pregnancy, or practice birth spacing, but
are not using contraception.
• Access to a wide range of contraceptive methods to
prevent unwanted pregnancy and help women to
practice birth spacing, including emergency
contraception where authorized, are effective
strategies for preventing future unwanted
pregnancies and unsafe abortion and helping women
achieve their reproductive goals.
25.
4. Reproductive andother health services
• Include reproductive and other health services
provided on-site at the facility where treatment has
taken place, or via referrals to other accessible
facilities.
• Reinforce connections among services and establish
mechanisms for ensuring that women in need get
them.
26.
26
Cont
Other health servicesmay include:
• STI/HIV prevention education, screening, diagnosis and treatment
• screening for sexual and/or domestic violence, immediate treatment as
needed, and referral for medical/social/economic services and support
• screening for anemia, and treatment and/or nutrition education
• infertility diagnosis, counseling and treatment
• nutrition education
• hygiene education
• cancer screening and referral, as needed
27.
5. Community andHealth care provider
partnership
• Community members play a vital role in reduction of
maternal morbidity and mortality and improving
women's sexual and reproductive health and lives.
• To achieve universal local access to sustainable,
high-quality PAC and other health services,
community members, lay health workers and
traditional healers and formally trained service
providers must work in partnership.
28.
Approach to apatient with abortion
Thorough history
• Last Menstrual Period (LMP)
• Gestational Age (GA)
• Gravidity and Parity
• Pregnancy symptoms
• Current complains (LAP, bleeding, discharge, fever, induction, etc)
28
29.
Medical History
• Priormanagement of the current abortion
• Asthma, heart disease
• Bleeding disorders
• Tetanus, Rh vaccinations
• Surgical history
• Physical, cognitive, mental disability
29
30.
Ob-Gyn History
• Pastpregnancies, outcomes
• STI, HIV status
• Contraceptive history
• Cervical cancer screening
30
31.
Physical Exam
General exam
•A complete physical exam should be performed
• Vital signs: blood pressure, temperature, pulse
rate, oxygen saturation
• General appearance: alertness and orientation,
paleness, jaundice, dyspnoeic, fever, in distress
(pain??)
31
32.
Physical exam
Abdominal exam
•Distensions, scars, signs of trauma, Soft, tenderness, rebound and
guarding, size of the uterus, any other masses, size of liver
Pelvic exam
• Bleeding, amount, clots, POC, discharge
• Speculum: Open/closed cervix, active bleeding, POC, discharge, signs
of trauma
• Bimanual exam: Uterine size and position, tenderness, cervical
excitation, adnexal mass and tenderness
32
Signs/Symptoms of SHOCK
•Current or recent excessive vaginal bleeding
• Fast pulse with low blood pressure
• Pale, cool skin but sweating
• Fast breathing
• Anxiety, restlessness
• Unconsciousness, feeling faint, or disoriented
• Shortness of breath
34
35.
Signs/Symptoms of SEPSIS
•Fever (38ºC or more)
• Chills, sweats (with or without fever)
• Feels very ill, close to collapse
• Fast pulse with low blood pressure
• Lower abdominal pain, bloating, nausea, diarrhea
• Shortness of breath/ respiratory distress
• Symptoms of pelvic infection
35
36.
Lab investigation
– Hemoglobinor hematocrit
– Full blood count more preferable
– Pregnancy testing
– Blood Grouping and RH testing
– Bed side clotting time
– PT and aPTT if available
– Creatinine, Urea
– CRP
36
37.
Management of patientwith abortion
• Depends on;
1. Patient status
2. Presence and amount of bleeding
3. Signs of sepsis
4. Type of abortion
38.
If patient isin shock
• Shout for help
• Apply ABCD
• Insert two large bore cannula
• Take blood for ivestigations
• IV fluids crystalloids (ration 1:3) or 3 litre in first hour
• Catheter
• If not CEmONC facility refer (folow protocol for transfer of severly ill
patients)
Contraindication to medical
management
•History of allergy to misoprostol or other
prostaglandins
• Patients with sepsis
• Suspicion of ectopic pregnancy
• Women with in IUD in place (once removed
woman is eligible)
• Patient who are hemodynamically unstable
• Severely bleeding women
42.
42
Manual Vacuum Aspiration
(MVA)
•Uses vacuum aspirator attached to cannula of different
sizes
• Simple cost effective
• Done in office/procedure room
• No general anesthesia required
• May need to dilate the cervix prior to the procedure
• For uterine size up to 12 weeks
Complications of MVA
•Complications are rare.
• However, possible complications include:
• Incomplete evacuation
• Cervical or uterine injury, such as perforation or
tearing
• Anesthesia complications
• Infection
• Hemorrhage
• Hematometra
44
45.
Surgical curettage
• Alsoknown as Dilatation & Curettage (D&C)
• For uterine size >12 weeks
• May involve dilating the cervix
• Uses Sharp metal curette
• Usually done under general anesthesia/heavy sedation
• More costly, prolonged procedural time, increased blood
loss
• Complications such as uterine perforation, hemorrhage,
pain, long term complications such as uterine synaechiae
45
46.
After the procedure
•Inspect the products of conception
• Insert IUCD
• Provide oral antibiotics
• Provide hematenics
• Provide the chosen contraception if not IUCD
• Process the equipment
• Discharge with follow up information
• Counsell danger sign and when to expect menses
#7 Significant trauma can cause pregnancy loss, While the developing embryo is relatively protected within the uterus in early pregnancy,
#8 Ascending infection causing chorioamnionitis causes first and sec trimester abortions
Infection---inflammation---cytokines,oxygen free radicals---- cytotoxicity--- direct effect on the uterus or the fetoplacental unit.





























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















