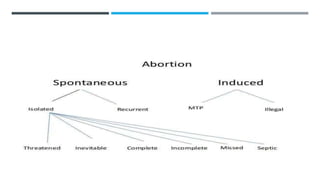
This document discusses abortion, including definitions, types, causes, and management. It begins by defining abortion and providing statistics on incidence. It then describes types of abortion, differentiating between spontaneous abortion (miscarriage) and induced abortion. Biological causes of spontaneous abortion are outlined, including fetal factors like genetic abnormalities and maternal factors like infections, endocrine issues, and anatomical abnormalities. The document also discusses legal issues surrounding abortion, challenges with access to services, and consequences of unsafe abortion. Approaches to addressing unsafe abortion, such as ensuring availability of services and training of health workers, are presented. Causes and management of unintended pregnancy as well as post-abortion care are also summarized.