Download to read offline
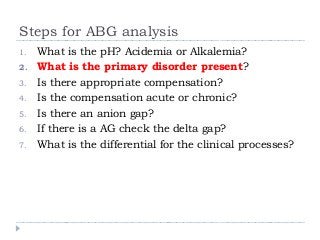
![Step 3-4: Is there appropriate
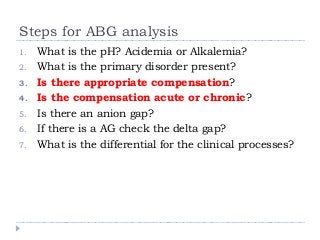
compensation? Is it acute or chronic ?
Metabolic Acidosis
Winter’s formula: pCO2 = 1.5[HCO3] + 8 ± 2 MEMORIZE
If serum pCO2 > expected pCO2 -> additional respiratory
acidosis
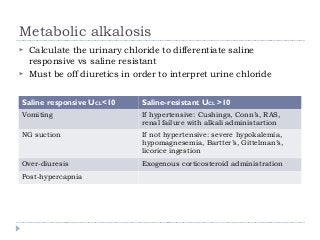
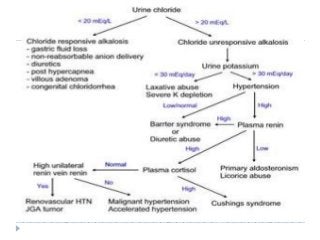
Metabolic Alkalosis
pCO2 = 0.9 [HCO3] + 9
For every 10 increase in HCO3 -> pCO2 increases by 6](https://image.slidesharecdn.com/abgptt-141027181202-conversion-gate01/85/ABG-ptt-27-320.jpg?cb=1733776075)
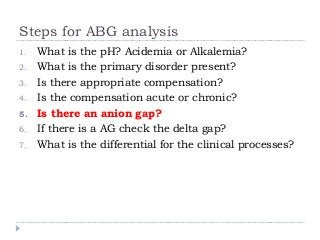
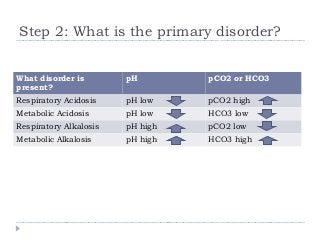
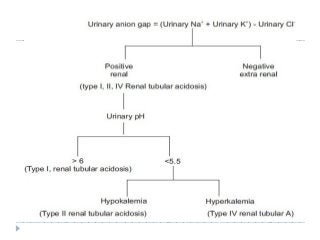
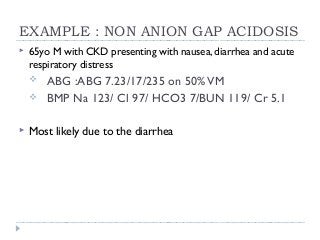
![Step 5: Calculate the anion gap
AG = Na – (Cl +HCO3 )(normal 12 ± 2)
AG corrected = AG + 2.5[4 – albumin]
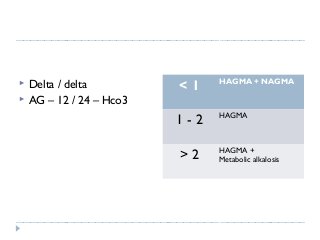
If there is an anion Gap then calculate the
Delta/delta gap (step 6). Only need to calculate
delta gap (excess anion gap) when there is an anion
gap to determine additional hidden metabolic
disorders (nongap metabolic acidosis or metabolic
alkalosis)
If there is no anion gap then start analyzing for
non-anion acidosis](https://image.slidesharecdn.com/abgptt-141027181202-conversion-gate01/85/ABG-ptt-30-320.jpg?cb=1733776075)



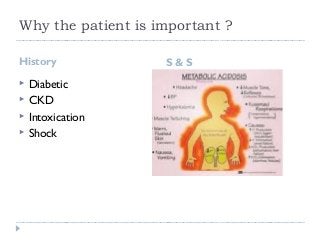
The document provides a comprehensive guide on arterial blood gas (ABG) analysis, emphasizing the importance of pH and key clinical conditions such as diabetic, respiratory, and shock scenarios. It outlines systematic steps for interpreting ABGs, including determining acid-base status, identifying primary disorders, and assessing compensation mechanisms. Additionally, it features various case studies to illustrate the application of ABG analysis in clinical settings.






















































