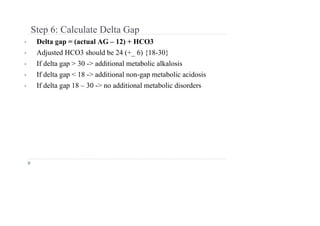
A blood gas analysis showed a pH of 7.27, pCO2 of 58 mmHg, and HCO3- of 26 mmol/L in a patient receiving 5L of oxygen. This represents a primary respiratory acidosis with appropriate chronic compensation, as the pH and pCO2 are low and HCO3- is elevated, consistent with long-standing respiratory acidosis. The anion gap and albumin are normal. This patient is experiencing chronic respiratory acidosis.


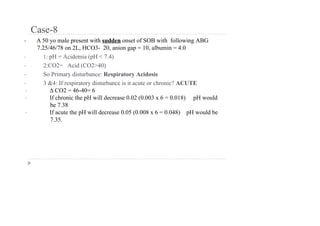
![CENTRAL EQUATION OF ACID-BASE
PHYSIOLOGY
➢ Henderson Hasselbach Equation:
➢ where [ H+] is related to pH by
• To maintain a constant pH, PCO2/HCO3- ratio should be constant
• When one component of the PCO2/[HCO3- ]ratio is altered, the
compensatory response alters the other component in the same direction to
keep the PCO2/[HCO3- ] ratio constant
● [H+] in nEq/L = 24 x (PCO2 / [HCO3 -] )
● [ H+] in nEq/L = 10 (9-pH)](https://image.slidesharecdn.com/arterialbloodgas-230627140630-07ba84d0/85/Arterial-Blood-Gas-ppt1-pdf-11-320.jpg)
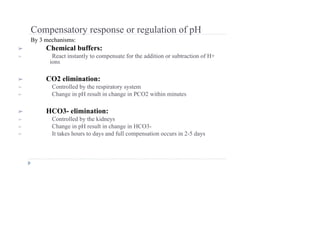
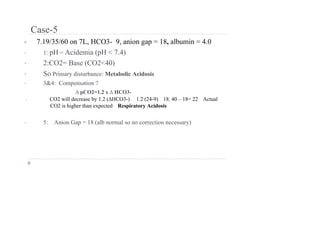
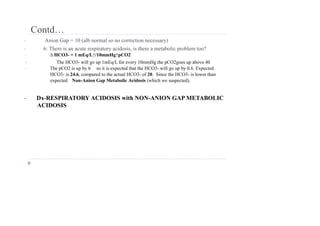
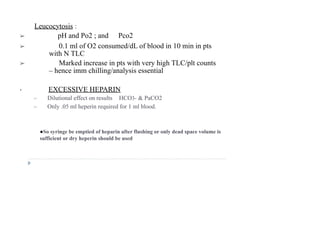
![EXPECTED CHANGES IN ACID-BASE DISORDERS
Primary Disorder Expected Changes
Metabolic acidosis PCO2 = 1.5 × HCO3 + (8 ± 2)
Metabolic alkalosis PCO2 = 0.7 × HCO3 + (21 ± 2)
Acute respiratory acidosis delta pH = 0.008 × (PCO2 - 40)
Chronic respiratory acidosis delta pH = 0.003 × (PCO2 - 40)
Acute respiratory alkalosis delta pH = 0.008 × (40 - PCO2)
Chronic respiratory alkalosis delta pH = 0.003 × (40 - PCO2)
From: THE ICU BOOK - 2nd Ed. (1998) [Corrected]](https://image.slidesharecdn.com/arterialbloodgas-230627140630-07ba84d0/85/Arterial-Blood-Gas-ppt1-pdf-20-320.jpg)
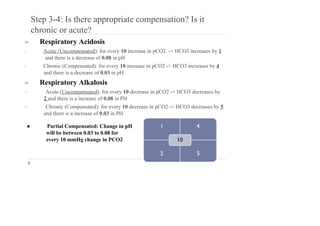
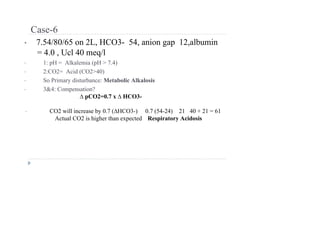
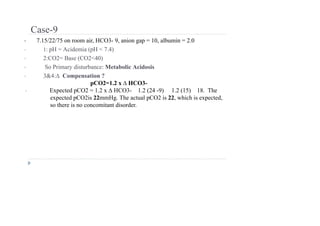
![Step 3-4: Is there appropriate compensation?
➢ Metabolic Acidosis
➢ Winter’s formula: Expected pCO2 = 1.5[HCO3] + 8 ± 2
OR
pCO2 = 1.2 ( HCO3)
➢ If serum pCO2 > expected pCO2 -> additional respiratory acidosis and
vice versa
➢ Metabolic Alkalosis
• Expected PCO2 = 0.7 × HCO3 + (21 ± 2)
OR
pCO2 = 0.7 ( HCO3)
• If serum pCO2 < expected pCO2 - additional respiratory alkalosis and
vice versa](https://image.slidesharecdn.com/arterialbloodgas-230627140630-07ba84d0/85/Arterial-Blood-Gas-ppt1-pdf-22-320.jpg)
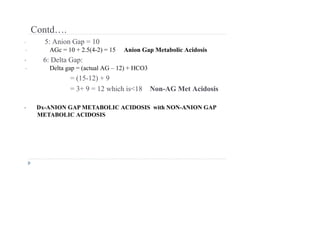
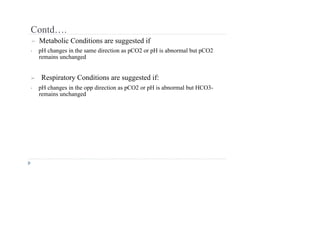
![Contd…
• AG corrected = AG + 2.5[4 – albumin]
• If there is an anion Gap then calculate the Delta/delta
gap (step 6) to determine additional hidden nongap
metabolic acidosis or metabolic alkalosis
• If there is no anion gap then start analyzing for non-
anion gap acidosis](https://image.slidesharecdn.com/arterialbloodgas-230627140630-07ba84d0/85/Arterial-Blood-Gas-ppt1-pdf-25-320.jpg)
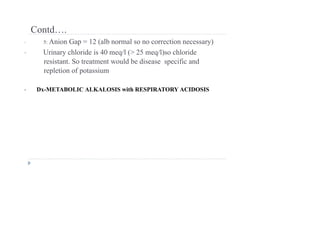
![EXAMPLE
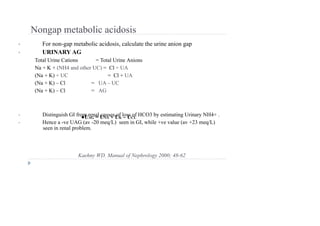
• Calculate Anion gap
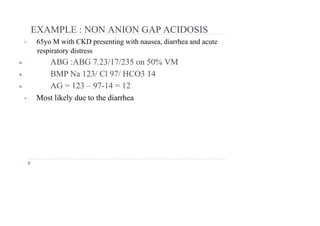
● ABG 7.23/17/235 on 50% VM
● BMP Na 123/ Cl 97/ HCO3 7/BUN 119/ Cr 5/ Albumin 2.
• AG = Na – Cl – HCO3 (normal 12 ± 2)
123 – 97 – 7 = 19
• AG corrected = AG + 2.5[4 – albumin]
= 19 + 2.5 [4 – 2]
= 19 + 5 = 24](https://image.slidesharecdn.com/arterialbloodgas-230627140630-07ba84d0/85/Arterial-Blood-Gas-ppt1-pdf-26-320.jpg)