Downloaded 14 times





















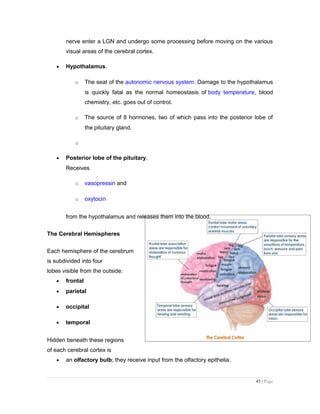
![The human brain receives nerve impulses from
• the spinal cord and
• 12 pairs of cranial nerves
o Some of the cranial nerves are "mixed", containing both sensory and
motor axons
o Some, e.g., the optic and olfactory nerves (numbers I and II) contain
sensory axons only
o Some, e.g. number III
that controls eyeball
muscles, contain motor
axons only.
The Hindbrain
The main structures of the hindbrain
(rhombencephalon) are the
• medulla oblongata
• pons and
• cerebellum
Medulla oblongata
The medulla looks like a swollen tip to the spinal cord. Nerve impulses arising here
• rhythmically stimulate the intercostal muscles and diaphragm — making
breathing possible.
• regulate heartbeat
• regulate the diameter of arterioles thus adjusting blood flow.
The neurons controlling breathing have mu (µ) receptors, the receptors to
which opiates, like heroin, bind. This accounts for the suppressive effect of opiates on
breathing.] Destruction of the medulla causes instant death.
42 | Page](https://image.slidesharecdn.com/formalgrandcasepresentation-130911072247-phpapp02/85/Formal-grand-case-presentation-42-320.jpg)





















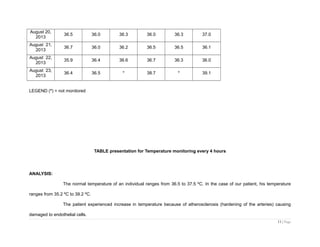
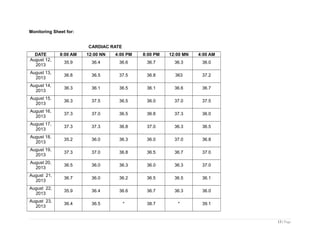
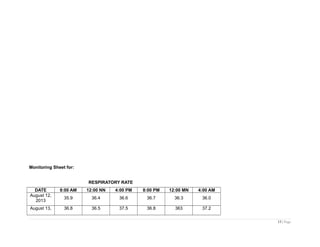
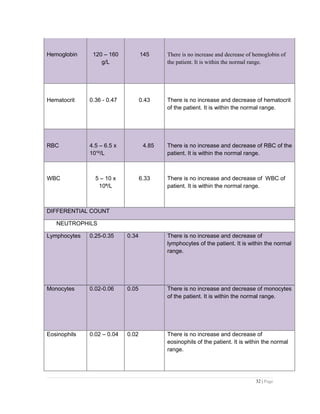
This document presents a case study of a 71-year-old female patient who experienced a stroke. It includes sections on the patient's history, including her past medical history of a previous stroke in 2005. Physical assessments were performed and vital signs such as temperature and cardiac rate were monitored daily. The document discusses the pathophysiology of stroke, medical management including medications and diagnostic tests, nursing care, and a discharge plan. The overall goal is to provide a clinical guide for a safe and quality nursing care approach for patients who experience stroke.



































![Pud Gastritis Lecture[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pudgastritislecture1-1232045267191333-1-thumbnail.jpg?width=640&height=640&fit=bounds)



















































