MD III Classof 2023
1st June 2021
Dr. Frank, FCOphth ECSA
Session 5
2.
INTRODUCTION
• Three formsare recognized (primarily a function of the Cone system:
• SPATIAL ACUITY: ability to resolve 2 points in space
• Location and Brightness effect
• Assessed using Snellen eye chart- relative to ability of the normal population to
distinguish the letter at 6 meters (6/6 vision is normal)
• TEMPORAL ACUITY: ability to distinguish visual events in time
• SPECTRAL ACUITY: ability to distinguish differences in the wavelength of the stimuli
3.
INTRODUCTION CONT’D…
• Humaneye is a complex optical instrument
• Properties may vary from person to person
• Several refractive surfaces with different refractive index
4.
VISUAL ACUITY (VA)
•In the visual system, Acuity refers to the ’ability to discriminate
fine details of the visual scene’
• An objective measure of what the person can see
• Tested at 6m/20ft using Snellen Charts: very little
accommodation
• Each eye tested separately, OD first
• Pinhole test (PH): simple optical test to detect refractive
errors
• Need for Near vision and Distance vision testing
• Is part of routine examination-all patients
6/7/2021 4
7.
REFRACTIVE SURFACES OFTHE EYE
• Air/cornea interface
• Cornea/aqueous
• Aqueous/anterior surface of the lens
• Posterior surface of the lens/vitreous
• But the major refracting surfaces
• Cornea and Lens
8.
REFRACTION AT THECORNEA
• The light entering the eye is refracted markedly at the anterior
surface of the cornea.
• Because of its curvature
• The RI difference between air(1) and
the cornea (1.37).
• The optical power of the human cornea is 40-45D
9.
REFRACTION AT THELENS
• The light undergoes little further refraction until it
reaches the lens at both surfaces of which is refracted.
• Lens makes sure the rays of light come to focus on the
retina.
• It focuses both near and distant objects by changing its
shape a process called accommodation
• The optical power of the human lens is 16-20D
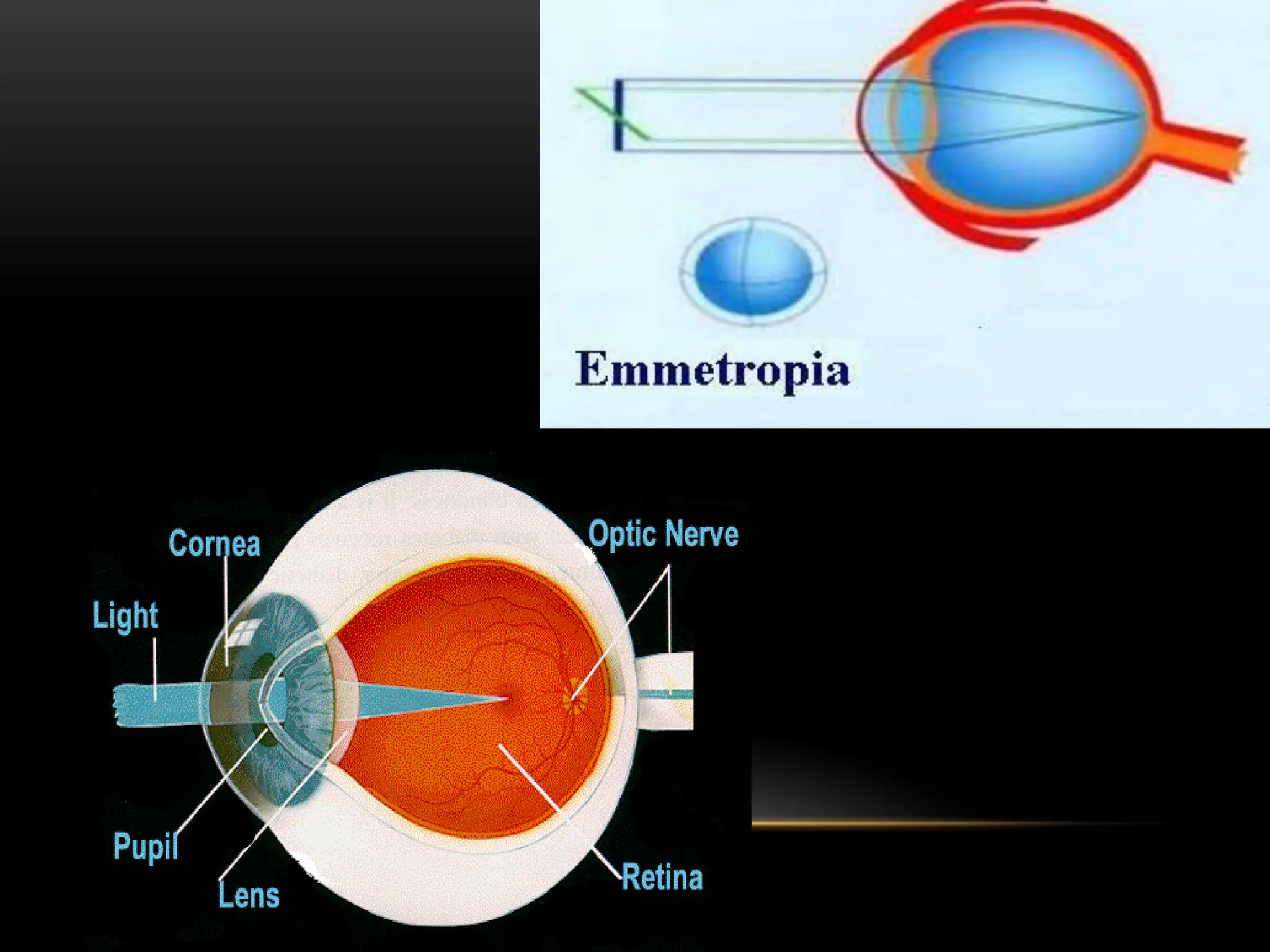
EMMETROPIC EYE
• Aneye without RE
• Parallel rays of light are brought to focus on the fovea without
the use of accommodation
13.
AMETROPIC EYE
• AnEye with Refractive Errors
• Refractive state of the eye is determined by Four
components:
• Corneal power (Mean, 43D)
• ACD (mean,3.4mm)
• Crystalline lens power (mean, 21D)
• Axial length (mean, 24)
14.
REFRACTIVE ERRORS
• Occurswhen the eye cannot clearly focus the images from the
outside world.
• The result of refractive errors is blurred vision, which is
sometimes so severe that it causes visual impairment.
• Uncorrected refractive error accounts for half of the global
burden of avoidable vision impairment and nearly a third of the
global burden of avoidable blindness.
• WHO estimates that 153 million people worldwide live with
visual impairment due to uncorrected refractive errors.
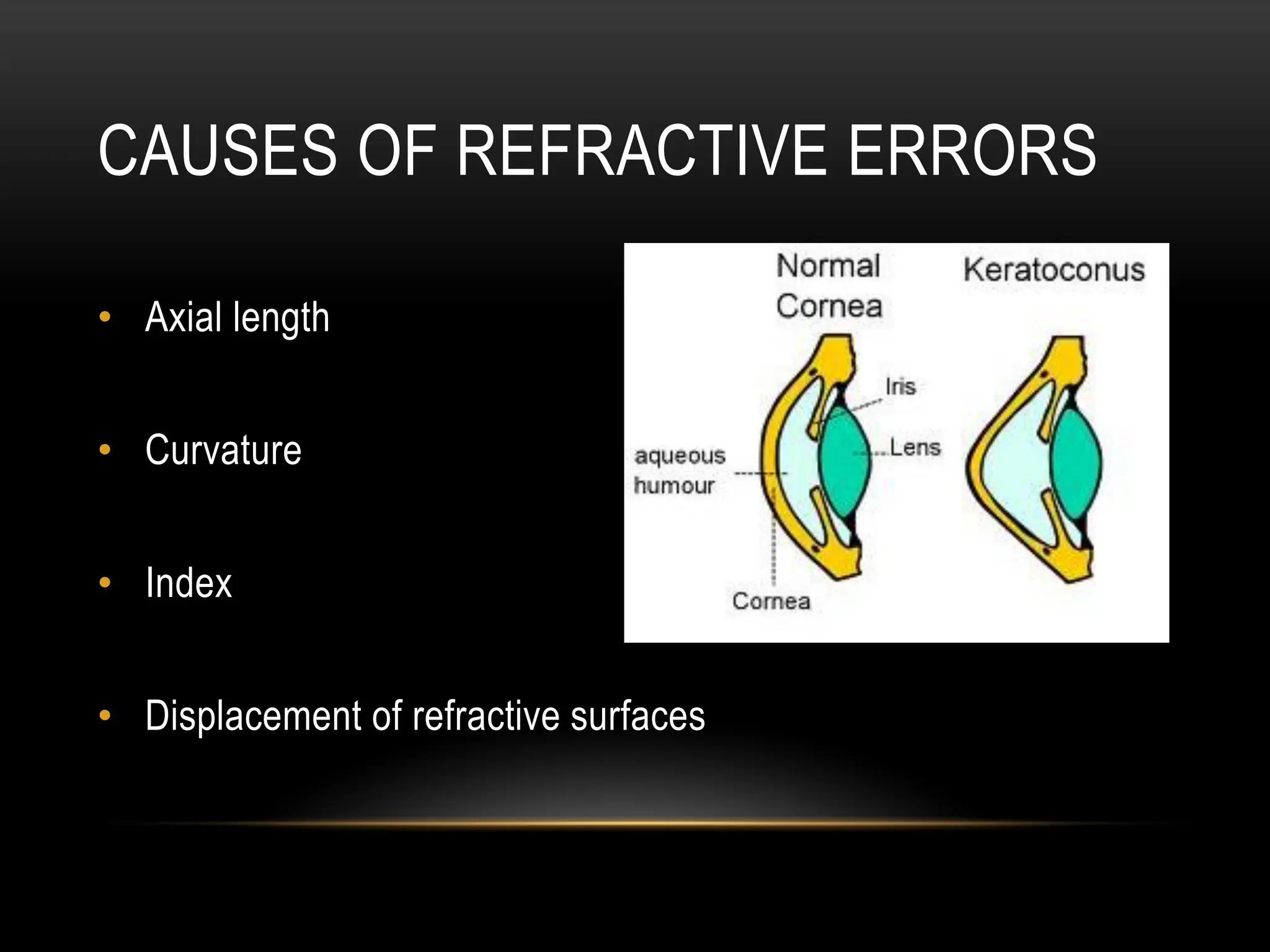
CAUSES OF REFRACTIVEERRORS
• Axial length
• Curvature
• Index
• Displacement of refractive surfaces
17.
DIAGNOSIS OF R.E
•History from patient: Cant see far/near/headaches/blurry
• Physical Examination: VA, IOP
• Retinoscope
• Pin Hole (For Screening)
• SLE
• Fundoscopy
• CVFT
18.
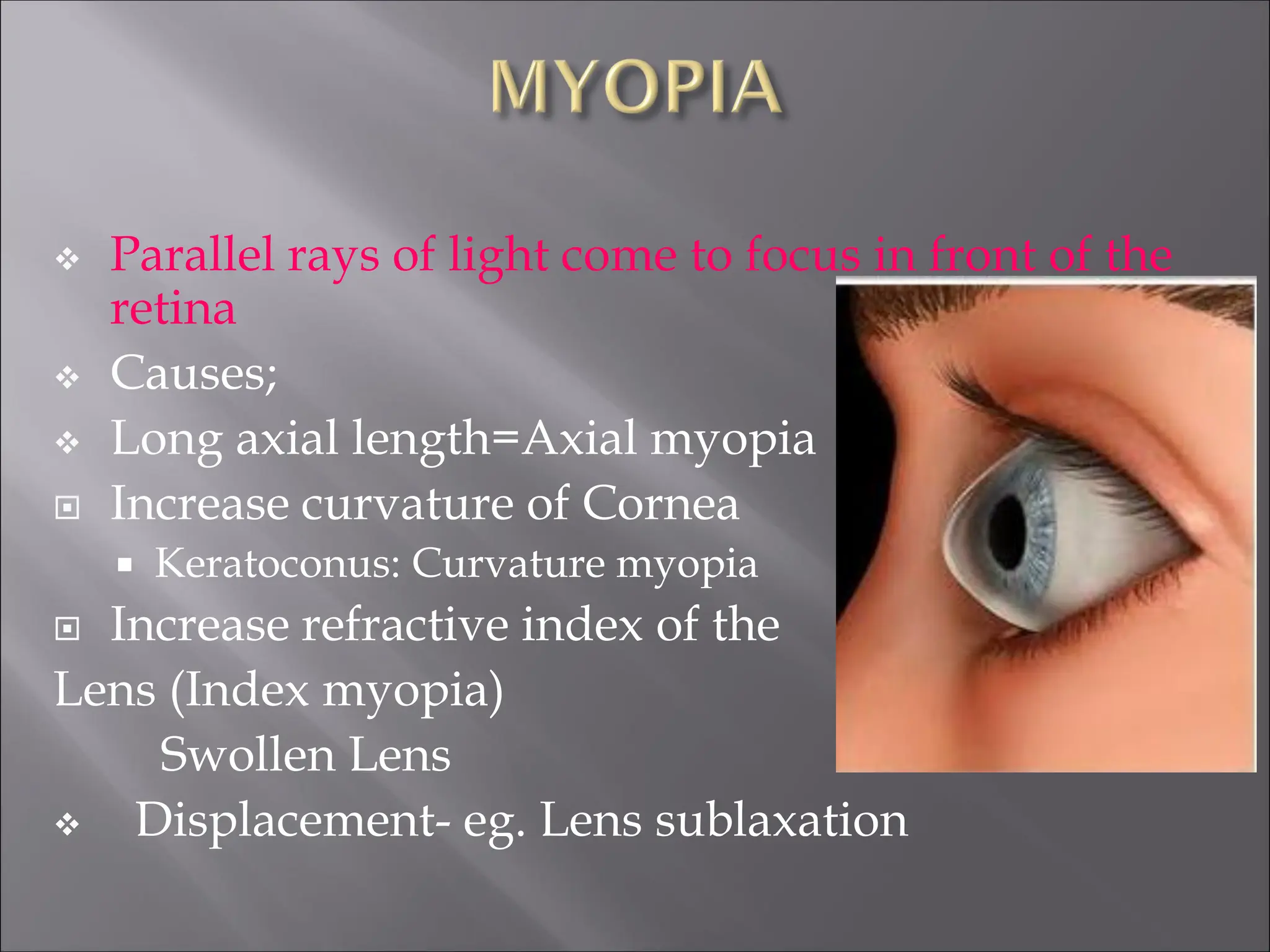
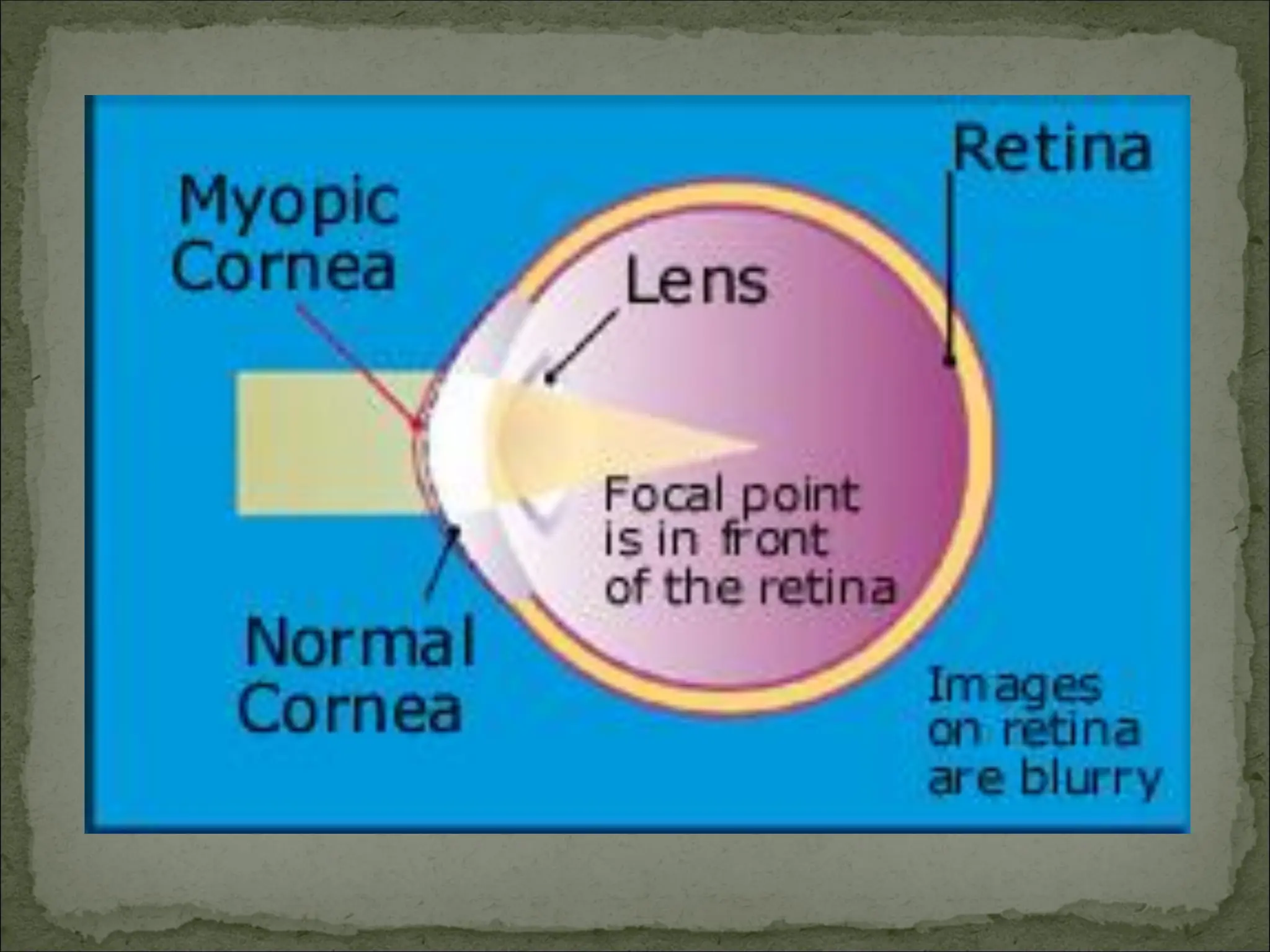
Parallel raysof light come to focus in front of the
retina
Causes;
Long axial length=Axial myopia
Increase curvature of Cornea
Keratoconus: Curvature myopia
Increase refractive index of the
Lens (Index myopia)
Swollen Lens
Displacement- eg. Lens sublaxation
20.
CLINICAL FEATURES
• Poordistant vision hence shortsighted
• Squinting
• Eyelid squeezing/ blinking
• Asthenopic symptoms
• Eye fatigue
• Headache
• Photophobia
o Pathological myopia(progressive)
o more than 6D
o 2% of population
o affects more females X2
Complications; Retinal hole, RD, degeneration
Hereditary: 10 - 25%
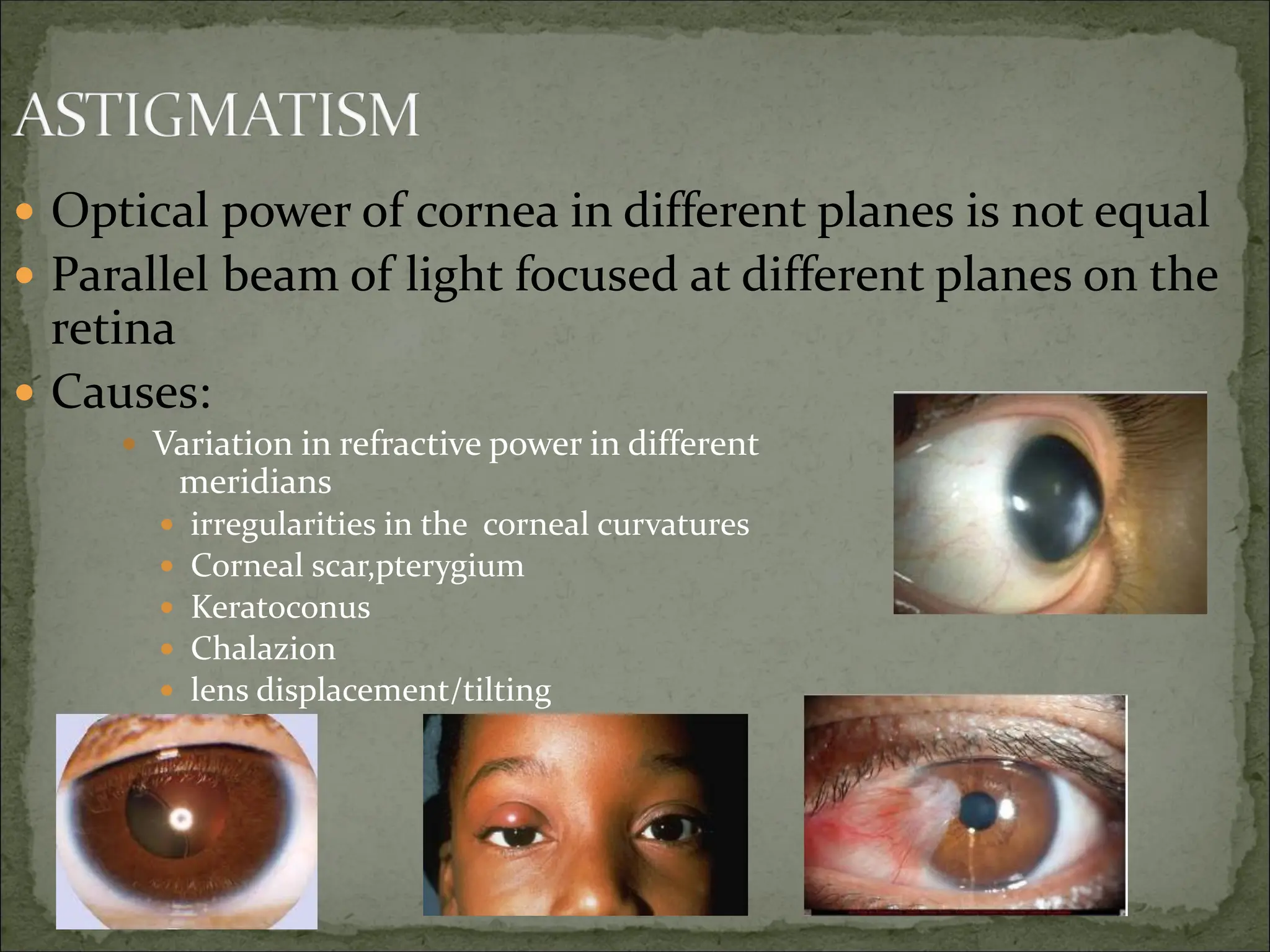
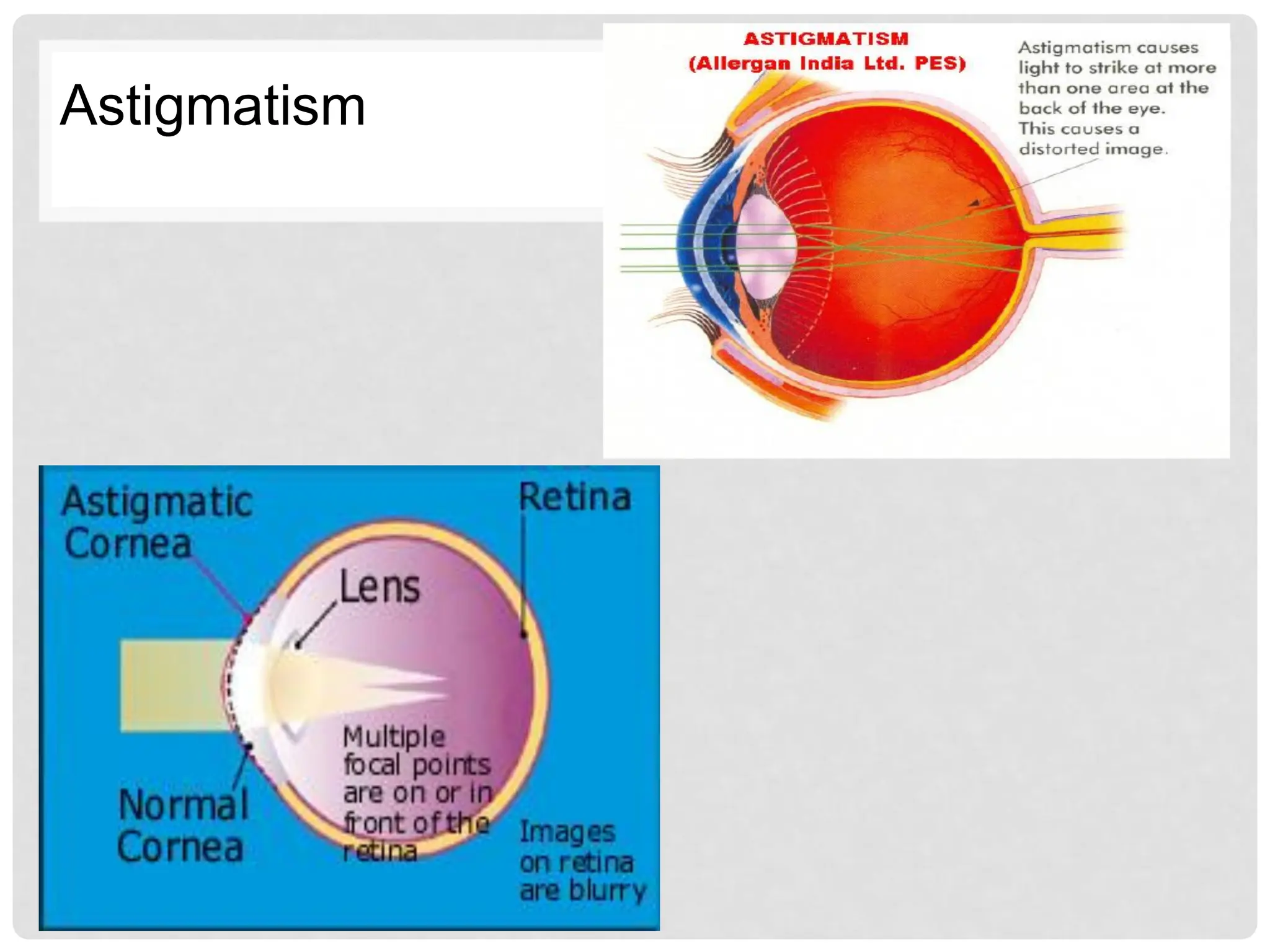
Optical powerof cornea in different planes is not equal
Parallel beam of light focused at different planes on the
retina
Causes:
Variation in refractive power in different
meridians
irregularities in the corneal curvatures
Corneal scar,pterygium
Keratoconus
Chalazion
lens displacement/tilting
SYMPTOMS AND TREATMENT
Symptoms
• Poor vision can be either at
distant or near
• Asthenopia
• Fatigue
• Headache
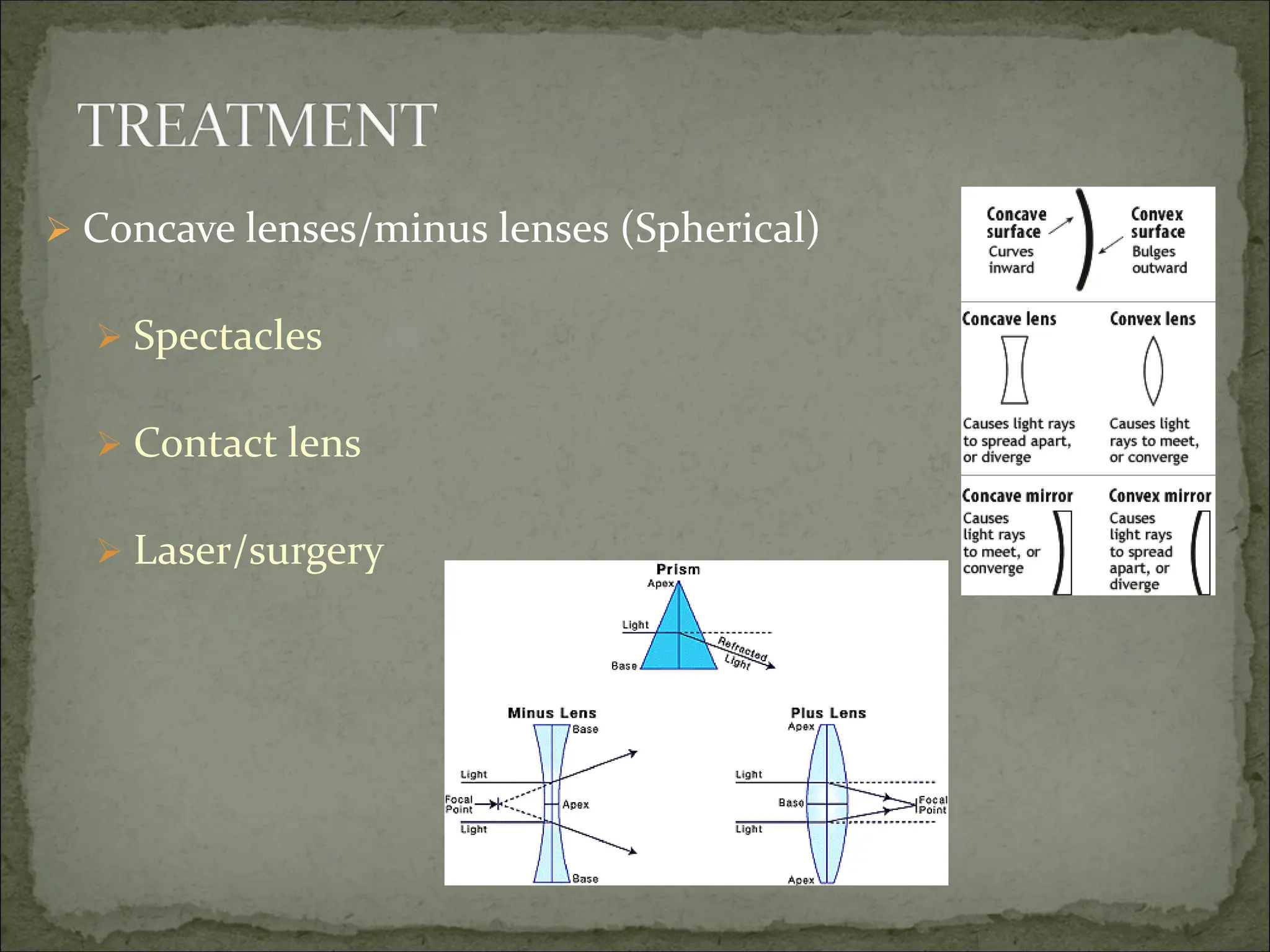
Treatment
• Cylinder lenses
• Spectacles
• Contact lens
• Corneal transplant
• Refractive Surgery
28.
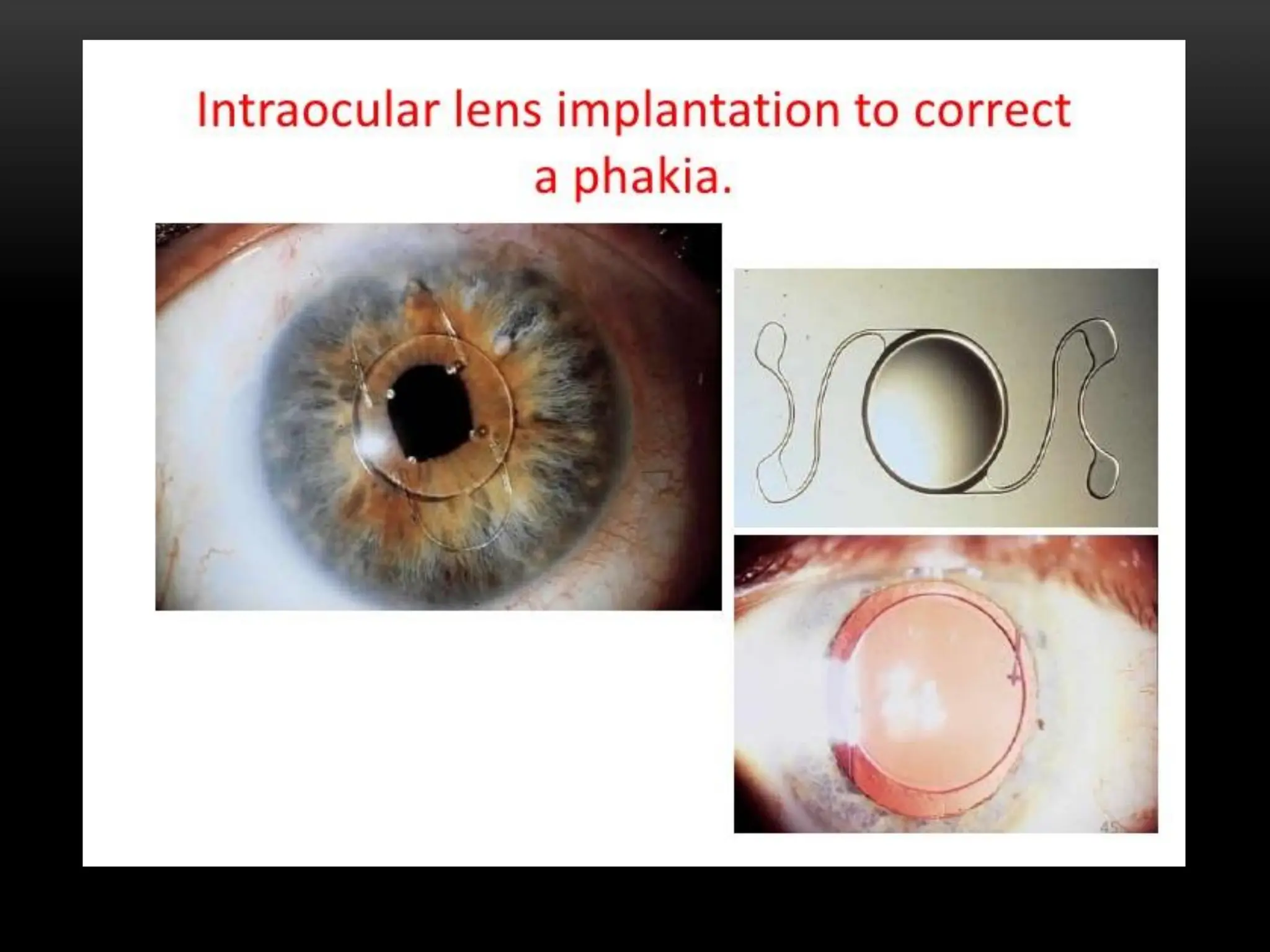
APHAKIA
• Absence ofthe natural lens
• Causes- surgical removal- commonest cause.
- trauma
- congenital absence
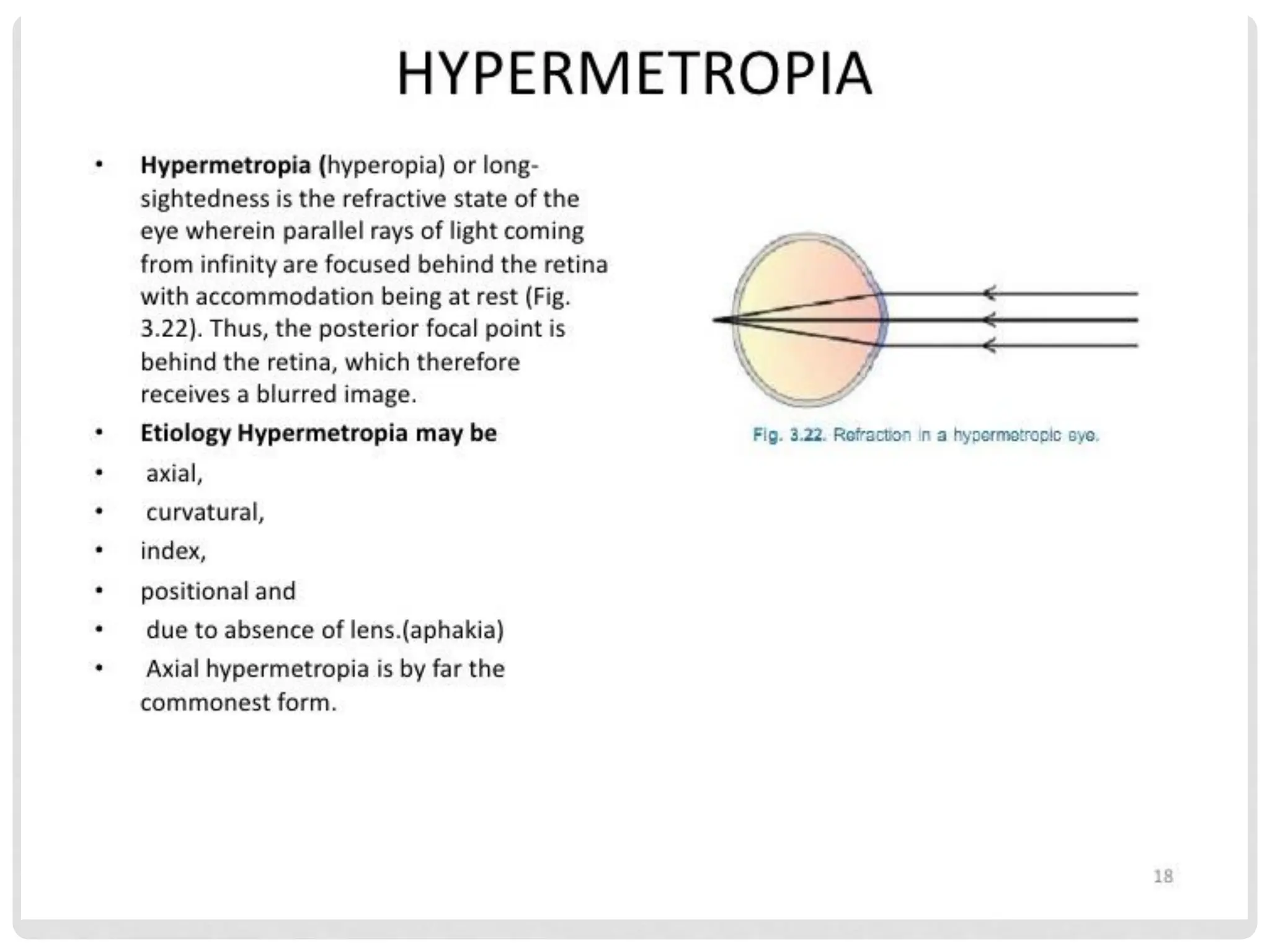
Symptoms- eye becomes highly hyperopic
- poor vision
- loss of accommodation
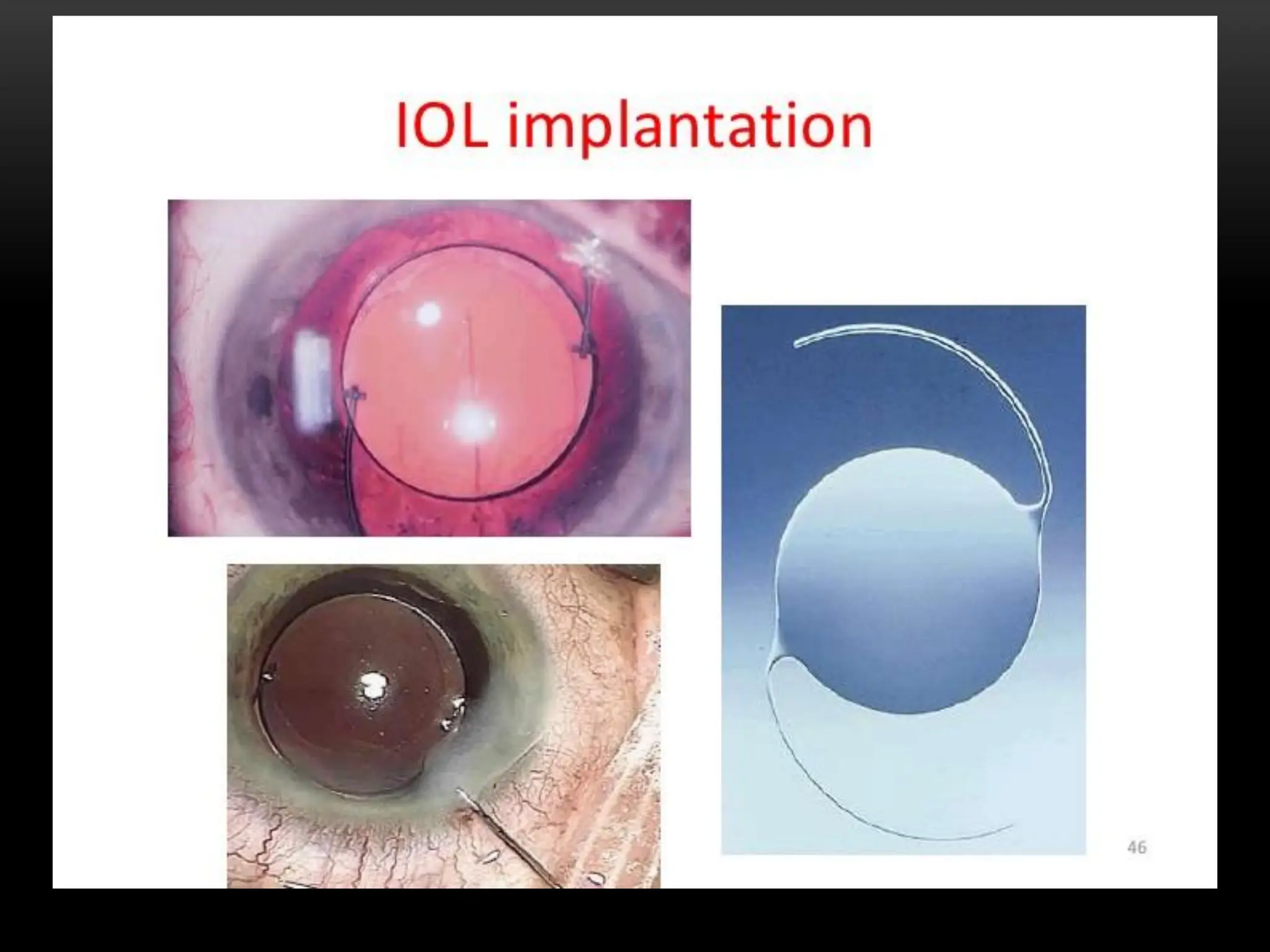
Treatment- aphakic spectacles/contact lens/IOL in P. Capsule,
Iris/Scleral fixation, AC
31.
PRESBYOPIA
Definition: lossof accommodation with age due to loss of
elasticity of the lens and weakness in the ciliary muscles
Symptoms –begin at the age of 40 years
- Inability to read small prints initially at near
- worse in dim illumination
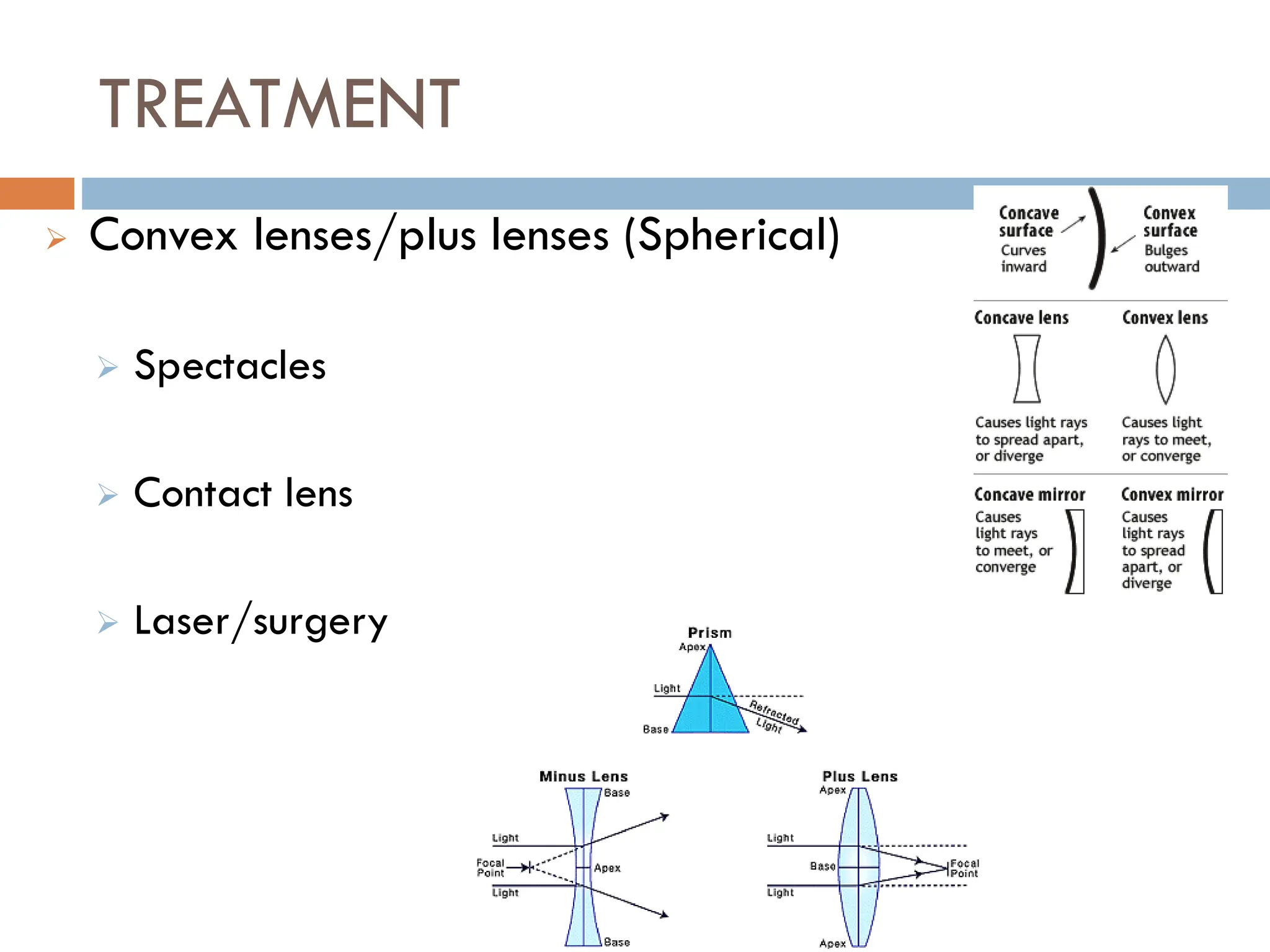
Treatment-reading glasses (convex lenses)
32.
SUMMARY
• Major Refractionsurfaces of the eye?
• Types of Lenses
• Types of RE
• Causes of RE
• Commonest?
• Diagnosis?
• Management?
• RE due to Old age?
Questions/Additions??
REFERENCE BOOKS FOROPHTHALMOLOGY
1. Brad Bowling, Kanski's Clinical Ophthalmology- A systematic
approach
2. Vaughan and Asbury's General Ophthalmology
3. Comprehensive Opthalmology by A. K Khurana
4. ABC of Eyes by Shah and Khaw
5. N.R.Galloway, et al - Common Eye Diseases and their
Management
6. Eye Diseases in Hot climates
7. Basic Ophthalmology: Essential for Medical Students