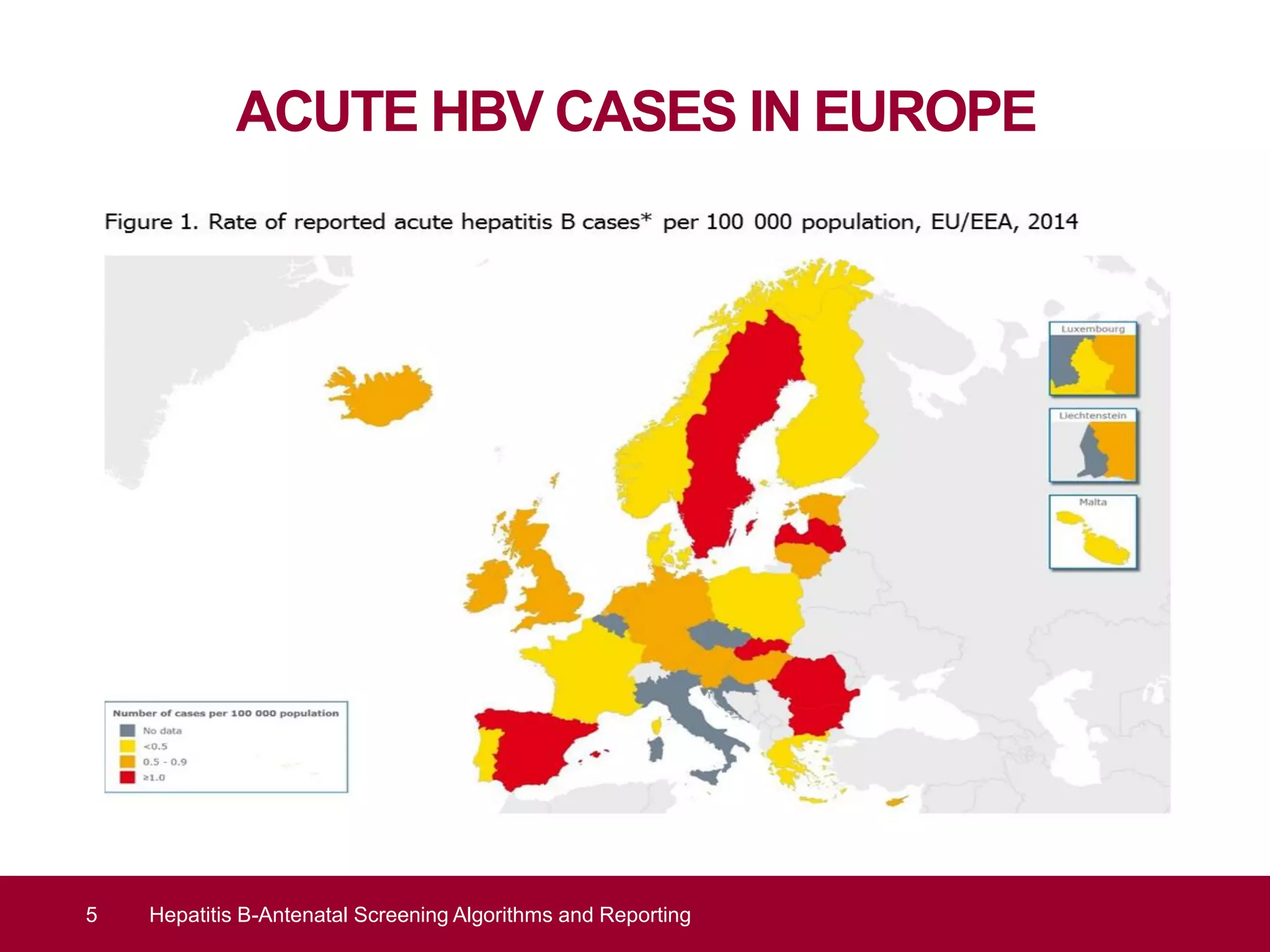
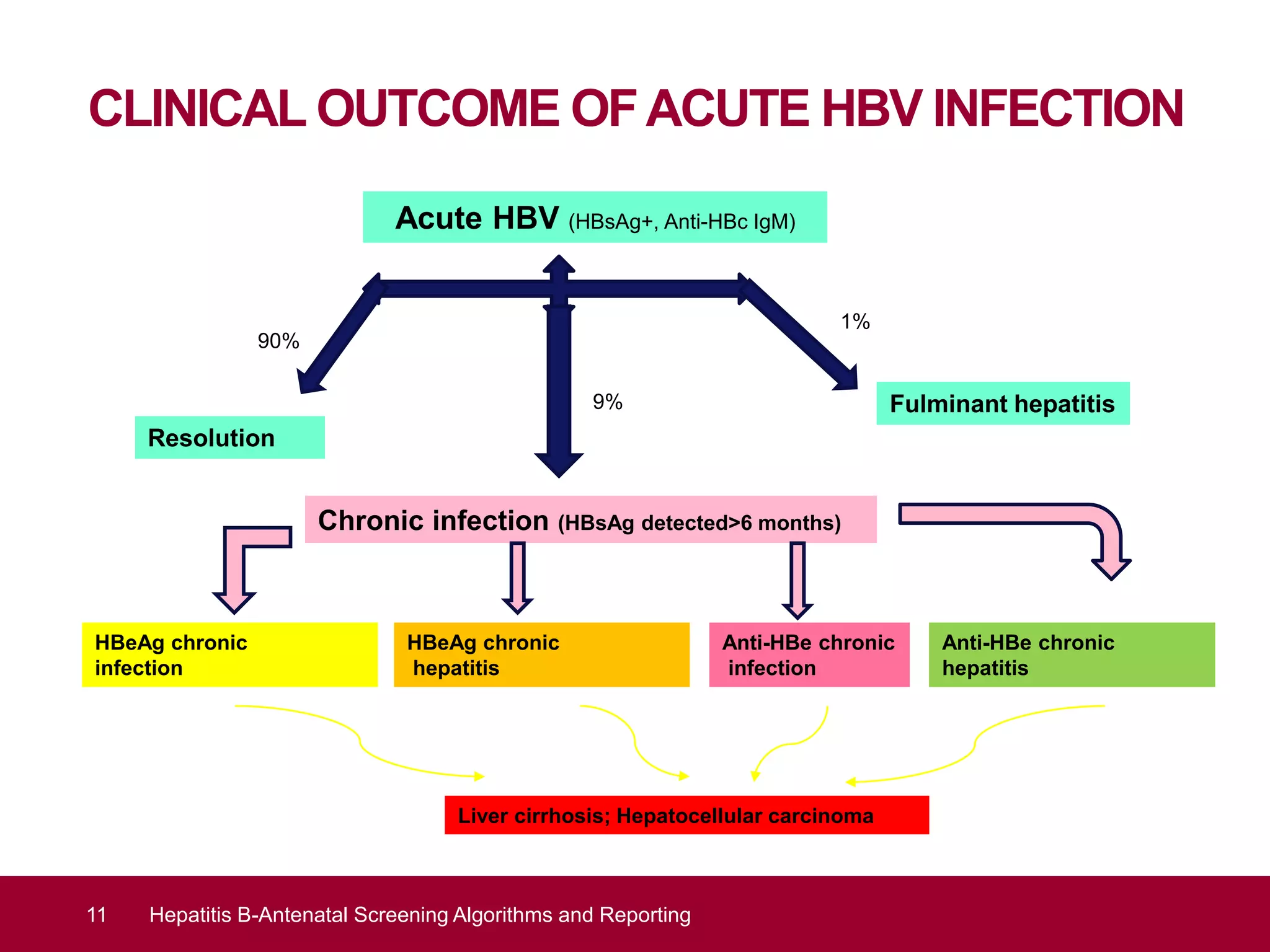
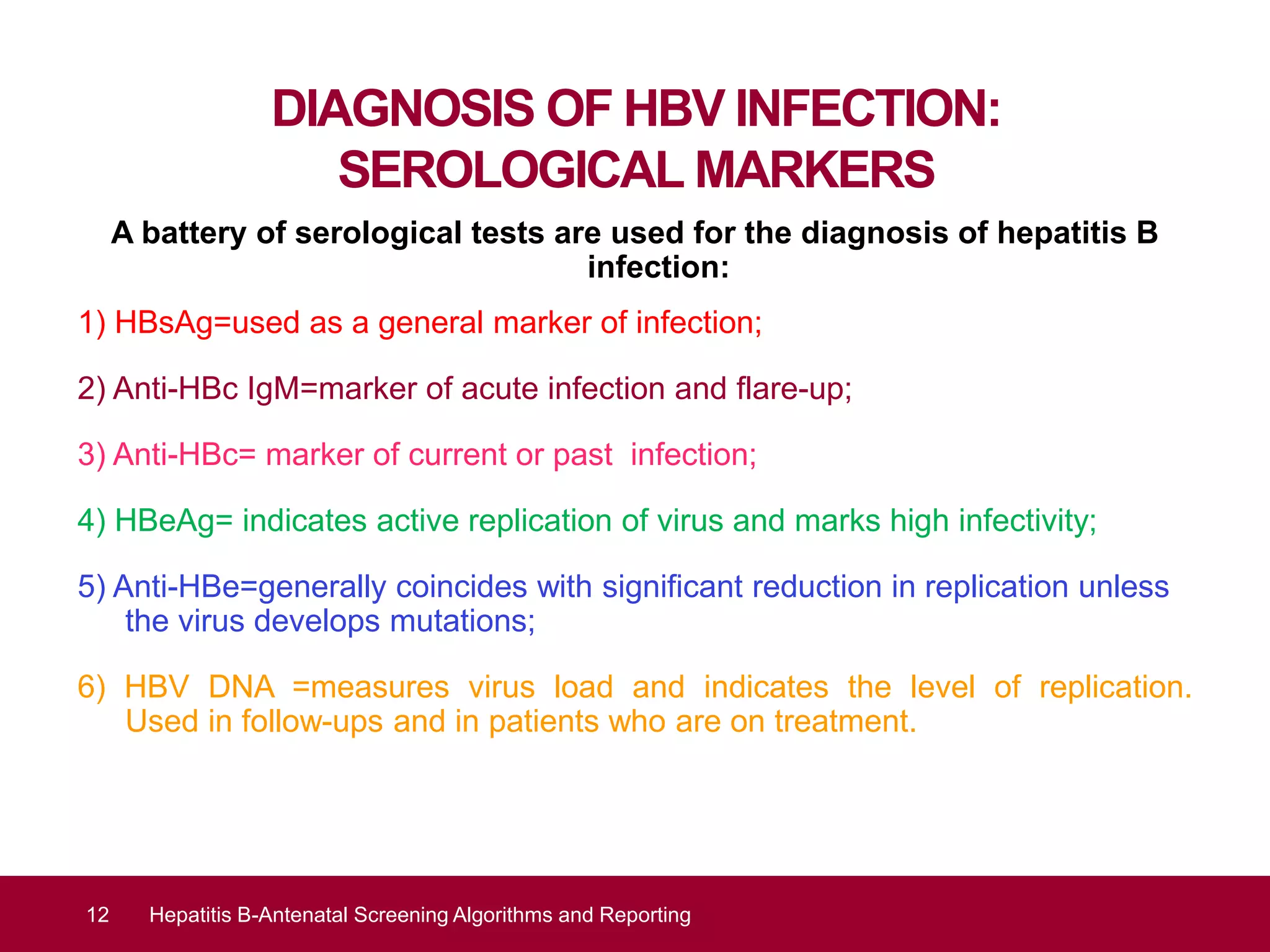
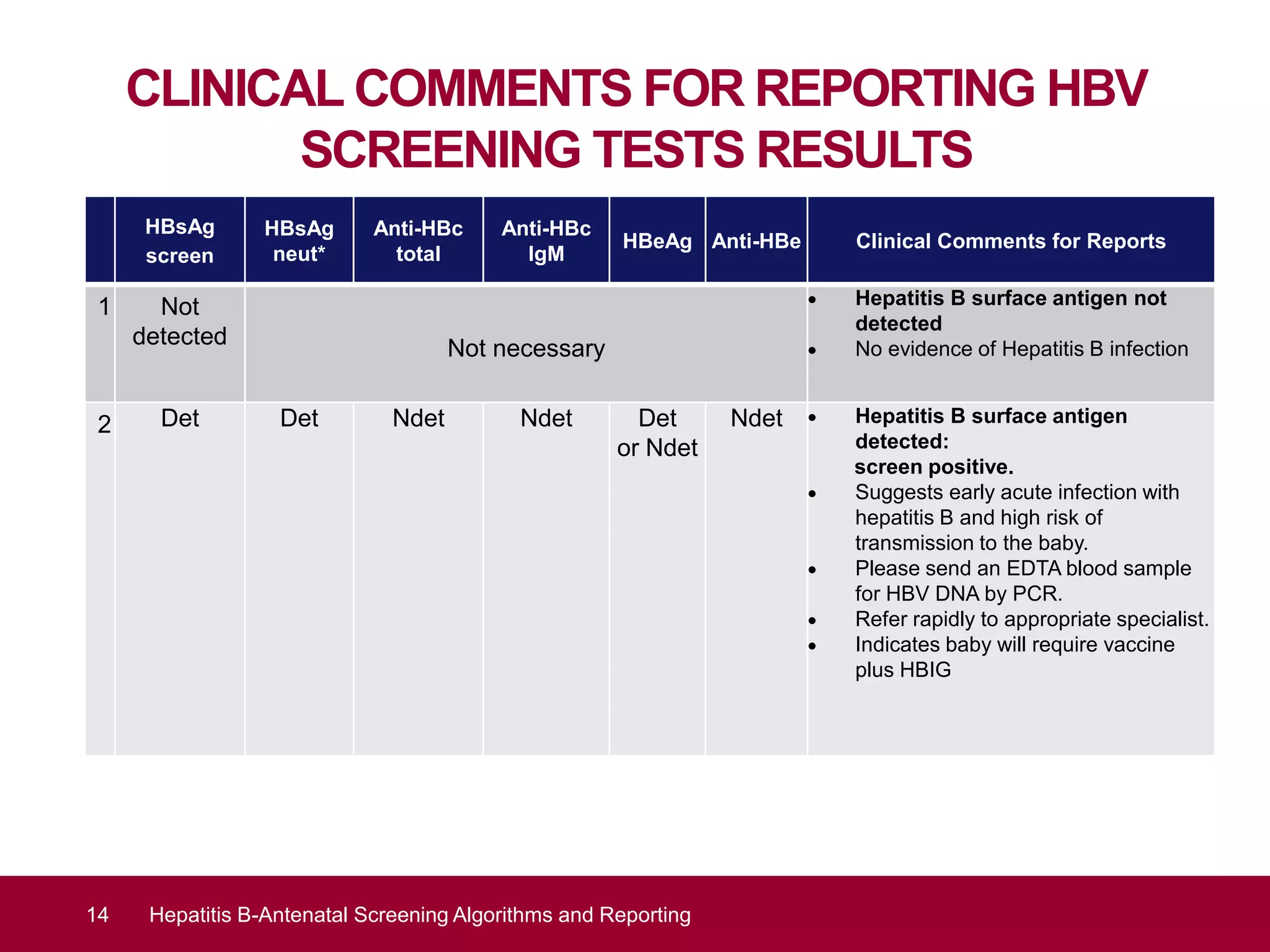
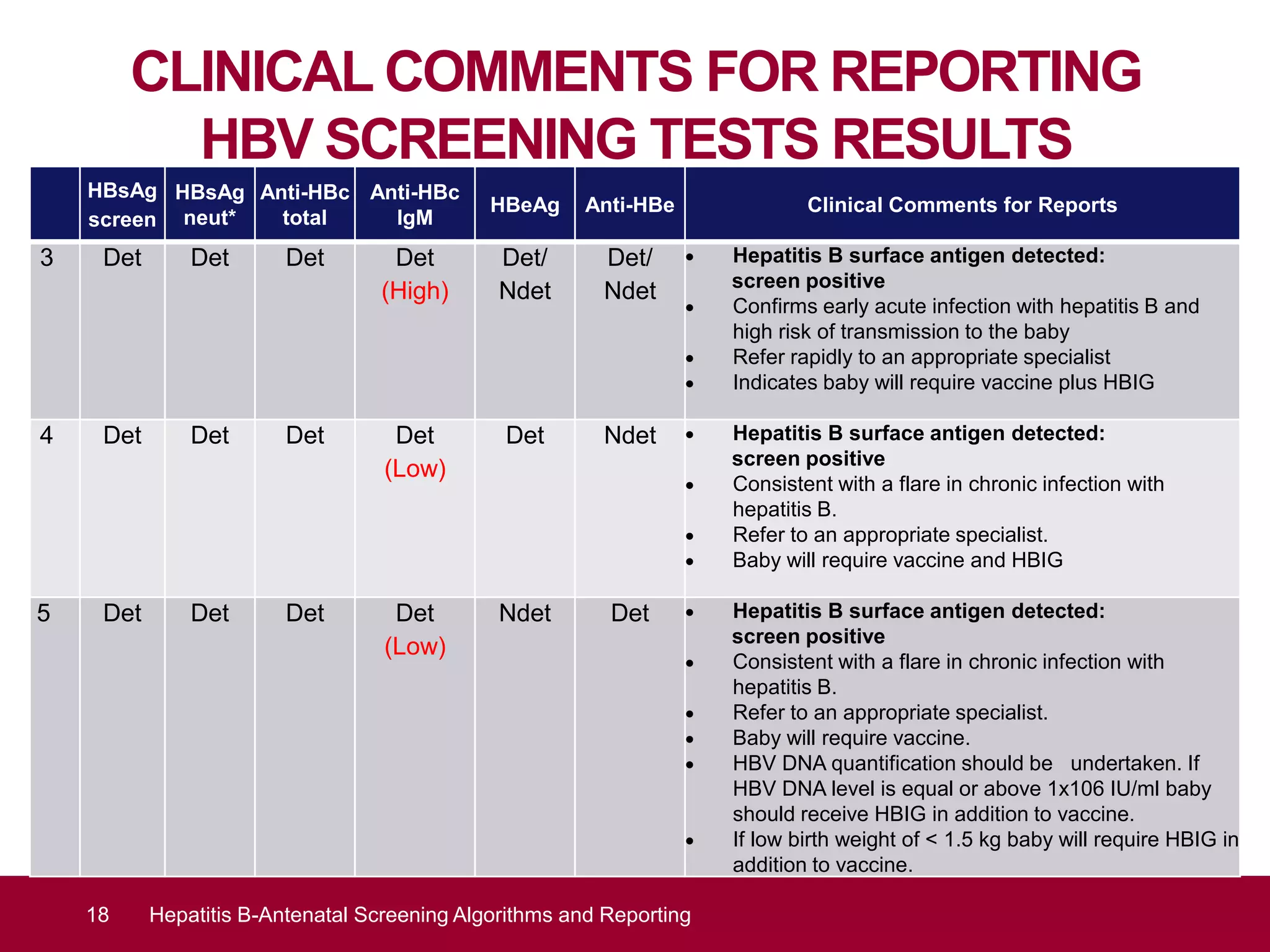
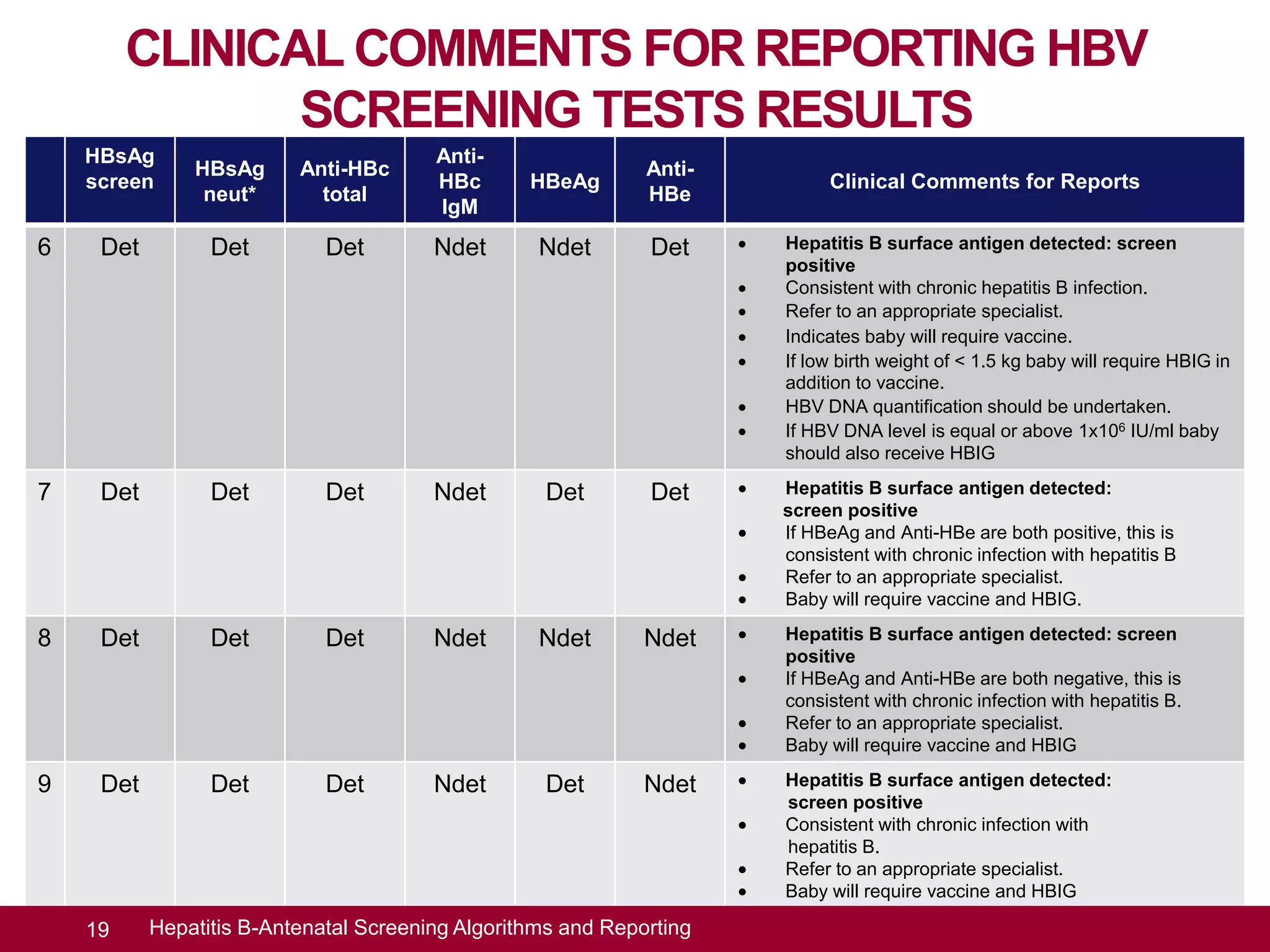
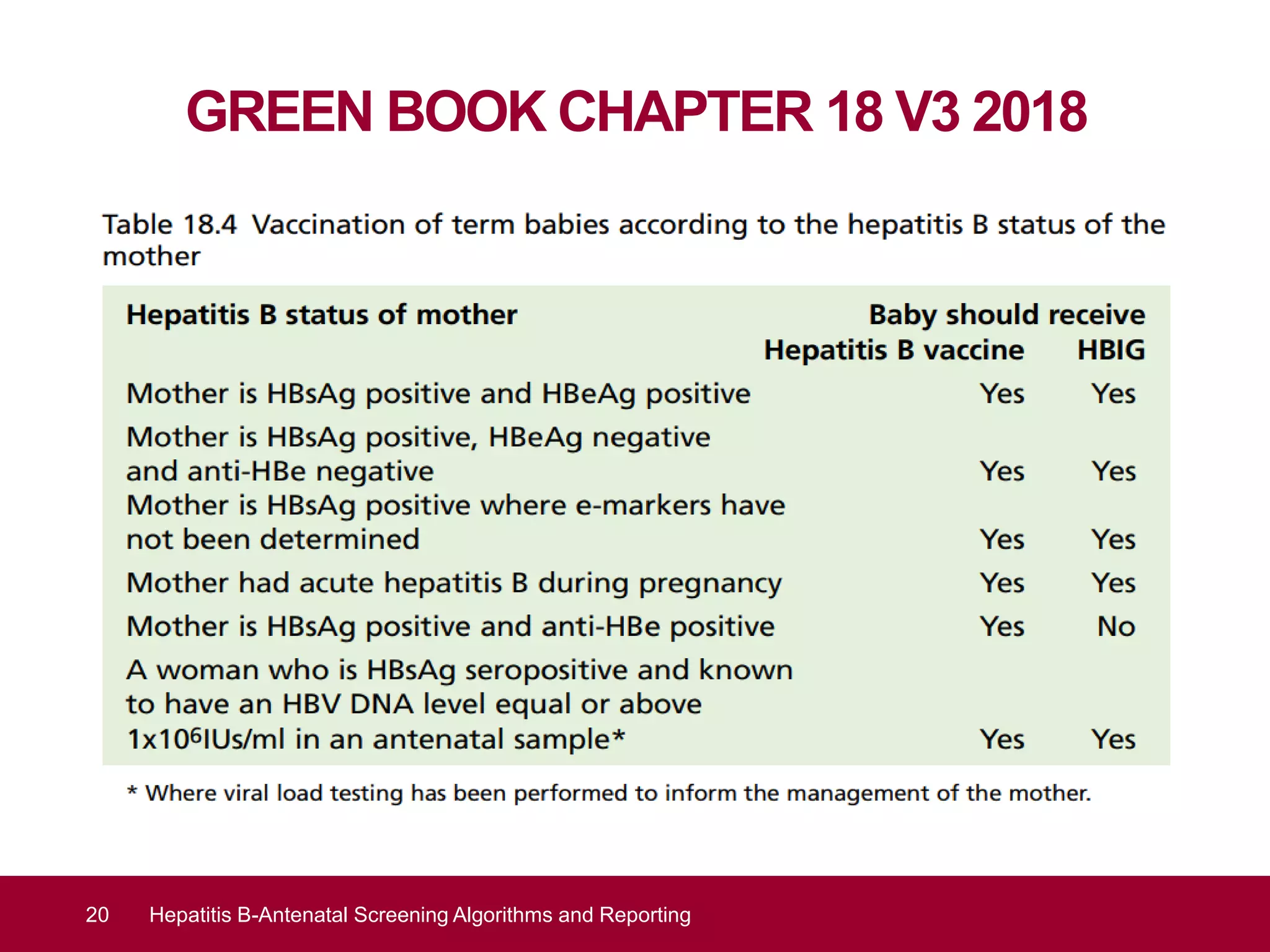
This document discusses hepatitis B screening algorithms and reporting for pregnant women in the UK. It provides background on the national screening program and standards for viral hepatitis B screening during pregnancy. The goals of antenatal hepatitis B screening are early detection of infection to enable treatment for the mother and reduce mother-to-child transmission risk by offering newborn vaccination and prophylaxis. The document reviews epidemiology data on acute hepatitis B cases in Europe and England and outlines the clinical outcome and diagnosis of hepatitis B infection through various serological markers. It presents the hepatitis B testing algorithm and provides clinical comments for reporting screening test results.