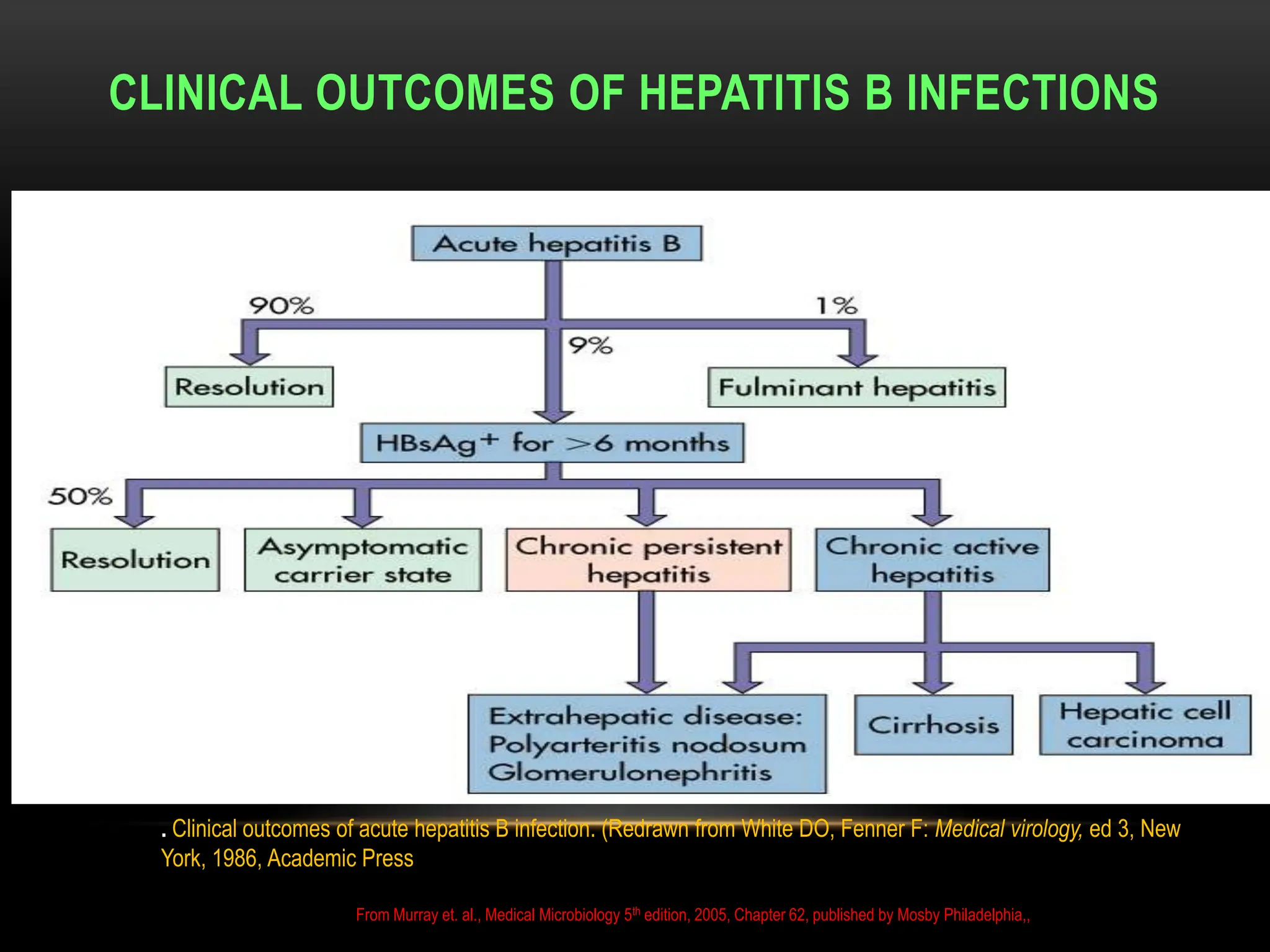
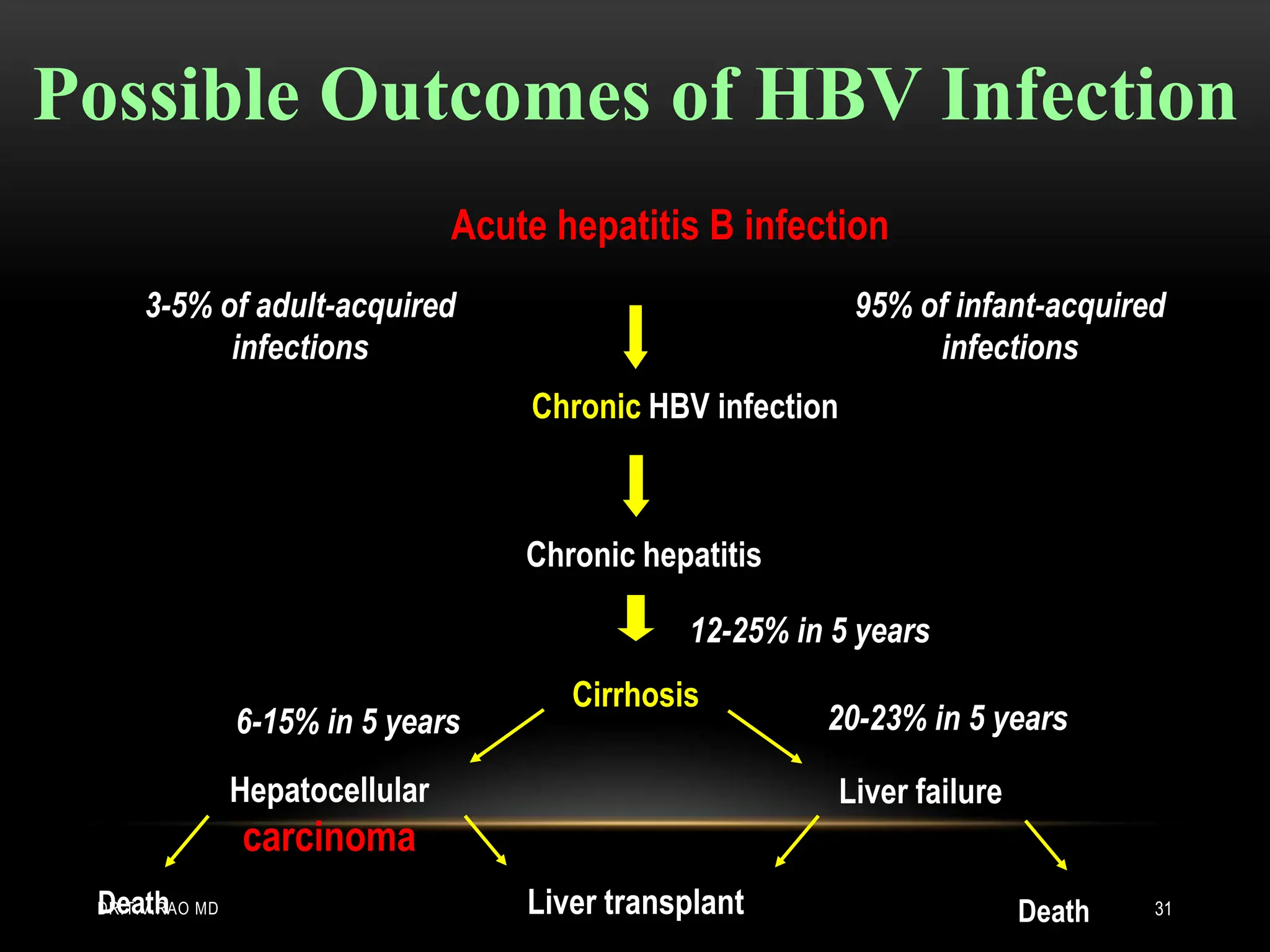
Hepatitis B infection affects approximately 2 billion people globally, with 400 million chronically infected, leading to about 1 million deaths annually. The document discusses the properties of the hepatitis B virus (HBV), its structure, serological markers, and the clinical outcomes of infections, including acute and chronic cases. It emphasizes the need for screening specific high-risk populations and outlines advanced diagnostic techniques for better management of HBV infection.