Downloaded 10 times
![105
Works Cited in Main Deck (2/15)
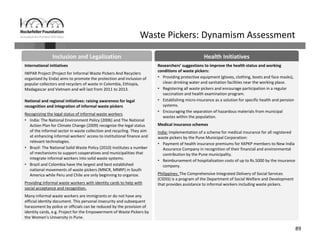
EXECUTIVE SUMMARY
• “Is Informal Normal? Messages, Figures and Data.” OECD. Accessed May 1, 2013.
http://www.oecd.org/dev/poverty/isinformalnormalmessagesfiguresanddata.htm.
• Mathauer, Inke, Jean‐Olivier Schmidt, and Maurice Wenyaa. “Extending Social Health Insurance to the Informal Sector in Kenya. An Assessment of Factors
Affecting Demand.” The International Journal of Health Planning and Management 23, no. 1 (March 2008): 51–68. doi:10.1002/hpm.914.
• Rani, Uma. Impact of Changing Work Patterns on Income Inequality. Discussion Paper. International Labour Organization, September 9, 2008.
http://www.ilo.org/inst/publication/discussion‐papers/WCMS_193166/lang‐‐en/index.htm.
• Rosenstock, Linda, Mark Cullen, and Marilyn Fingerhut. “Occupational Health.” In Disease Control Priorities in Developing Countries, 1127–1145. 2nd ed.
Washington, DC: The World Bank, 2006.
• The World Bank. (2013). World Development Indicators: Labor Force ‐ total [Data file]. Retrieved from
http://data.worldbank.org/indicator/SL.TLF.TOTL.IN.
• International Labor Organization and Women in Informal Employment: Globalizing and Organizing. (2012). Women and men in the informal economy ‐ A
statistical picture. [Data file]. Retrieved from http://www.ilo.org/global/statistics‐and‐databases/WCMS_179795/lang‐‐en/index.htm.
PROBLEM ASSESSMENT
• “Asiye Etafuleni |.” Accessed May 4, 2013. http://www.aet.org.za/.
• Barrientos, Stephanie. The ETI Code of Labor Practice: Do Workers Really Benefit? (South Africa). University of Sussex, United Kingdom: Institute of
Development Studies, 2006. http://www.ethicaltrade.org/sites/default/files/resources/Impact%20assessment%202c%20safrica.pdf.
• Benach, Joan, Carles Muntaner, Vilma Santana, and F. Chairs. “Employment Conditions and Health Inequalities.” Final Report to the WHO Commission on
Social Determinants of Health (CSDH) Employment Conditions Knowledge Network (EMCONET). Geneva: WHO (2007).
http://cdrwww.who.int/entity/social_determinants/resources/articles/emconet_who_report.pdf.
• Chen, Martha Alter, Renana Jhabvala, and Frances Lund. Supporting Workers in the Informal Economy : a Policy Framework. Working Paper. Working
Paper on the Informal Economy. International Labor Office, 2002. http://www.ilo.org/wcmsp5/groups/public/‐‐‐
ed_emp/documents/publication/wcms_122055.pdf.
• “Domestic Workers in the Informal Economy | WIEGO.” WIEGO. Accessed May 3, 2013. http://wiego.org/informal‐economy/occupational‐
groups/domestic‐workers#size.
• Dror, David, Van Putten‐Rademaker, and Ruth Koren. “Cost of Illness: Evidence from a Study in Five Resource‐poor Locations in India.” Available at SSRN
1016701 (2008). http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1016701.](https://image.slidesharecdn.com/37442dc9-fd4a-4fbb-b460-904888b88f57-external-150309101532-conversion-gate01/85/Health-Vulnerabilities-of-Informal-Workers-105-320.jpg)
![107
Works Cited in Main Deck (4/15)
PROBLEM ASSESSMENT CONT’D
• “RSBY: Rashtriya Swasthya Bima Yojna.” Accessed May 4, 2013. http://www.rsby.gov.in/.
• Smith, Peggie. “The Pitfalls of Home: Protecting the Health and Safety of Paid Domestics.” Canadian Journal of Women & the Law Washington University
in St. Louis Legal Studies Research Paper No. 11–03–03 (March 1, 2011): 40.
• “Statistical Picture | WIEGO.” WIEGO. Accessed May 1, 2013. http://wiego.org/informal‐economy/statistical‐picture.
• Taswell, K. 2001. “Using household surveys to collect basic information on occupational injuries.” Asian‐Pacific Newsletter on Occupational Health and
Safety, 8:34‐37.
• “Universal Coverage Scheme | Joint Learning Network for Universal Health Coverage.” Accessed May 4, 2013.
http://jointlearningnetwork.org/content/universal‐coverage‐scheme.
• van Niftrik, M., Reijnierse, J., Bogaard, A. and Lumens, M. (2003) ‘Occupational health and safety in the urban informal economy in Delft, South Africa’
African Newsletter on Occupational Health and Safety 13:13‐15
• Vanek, Joann, and Martha Chen. Women and Men in the Informal Economy: A Statistical Picture. International Labour Organization and WIEGO, 2012.
http://www.ilo.org/dyn/infoecon/docs/441/F596332090/women%20and%20men%20stat%20picture.pdf.
SCALE AND SCOPE
• Asian Development Bank, Informal Sector and Informal Employment in Bangladesh, 2010
• Asian Development Bank, The Informal Sector and Informal Employment in Indonesia, 2010
• Jacques Charmes, On Measuring Place of Work, Working paper, January 1, 2002, http://www.ilo.org/global/statistics‐and‐databases/WCMS_087887/lang‐
‐en/index.htm.
• Domestic Workers Across the World: Global and Regional Statistics and the Extent of Legal Protection (Geneva: International Labour Office, January 2013),
http://www.ilo.org/wcmsp5/groups/public/‐‐‐dgreports/‐‐‐dcomm/‐‐‐publ/documents/publication/wcms_173363.pdf.
• Kalpana Hiralal, “The ‘Invisible’ Workers of the Informal Economy–A Case Study of Home‐based Workers in Kwazulu/Natal, South Africa,” J Soc Sci 23, no.
1 (2010): 29–37.
• “Is Informal Normal? Messages, Figures and Data.” OECD. Accessed May 1, 2013.
http://www.oecd.org/dev/poverty/isinformalnormalmessagesfiguresanddata.htm.
• International Labor Organization and Women in Informal Employment: Globalizing and Organizing. (2012). Women and men in the informal economy ‐ A
statistical picture. [Data file]. Retrieved from http://www.ilo.org/global/statistics‐and‐databases/WCMS_179795/lang‐‐en/index.htm.](https://image.slidesharecdn.com/37442dc9-fd4a-4fbb-b460-904888b88f57-external-150309101532-conversion-gate01/85/Health-Vulnerabilities-of-Informal-Workers-107-320.jpg)
![108
Works Cited in Main Deck (5/15)
SCALE AND SCOPE CONT’D
• International Labour Organization, Decent Work for Women and Men in the Informal Economy: Profile and Good Practices in Cambodia, 2006
• International Labour Organization, Research on informal employment in Vietnam: current situation and solution, 2011.
• International Labour Organization, Vision for Asia’s Decent Work Decade: Sustainable Growth and Jobs to 2015, 2007.
• “Labor Markets ‐ Workers in the Informal Economy.” The World Bank. Accessed May 1, 2013.
http://web.worldbank.org/WBSITE/EXTERNAL/TOPICS/EXTSOCIALPROTECTION/EXTLM/0,,contentMDK:20224904~menuPK:584866~pagePK:148956~piPK
:216618~theSitePK:390615,00.html.
• Mohapatra, Kamala, Women Workers in Informal Sector in India: Understanding the Occupational Vulnerability. International Journal of Humanities and
Social Science, 2012.
• “MPI Data Hub Graph.” Migration Policy Institute Data Hub. Accessed May 1, 2013.
http://www.migrationinformation.org/DataHub/charts/worldstats_1.cfm.
• Naik, Ajaya, Informal Sector and Informal Workers in India, 2009.
• National Commission for Enterprises in the Unorganised Sector, Contribution of the Unorganised sector to GDP Report of the Sub Committee of a NCEUS
Task Force, 2008.
• Ratna M. Sudarshan and Renana Jhabvala, “Social Protection for Home‐Based Women Workers in South Asia: Learning from Action and Research” (2009),
http://dspace.cigilibrary.org/jspui/handle/123456789/21078.
• Ratna M. Sudarshan and Shalini Sinha, “Making Home‐Based Work Visible: A Review of Evidence from South Asia” (2011),
http://wiego.org/sites/wiego.org/files/publications/files/Sudarshan_WIEGO_WP19.pdf.
• Rockefeller Foundation, Informal City Dialogues: Bangkok’s webpage, http://nextcity.org/informalcity/city/bangkok.
• Shalini Sinha, Rights of Home‐based Workers (New Delhi, India: National Human Rights Commission, 2006), http://www.bhrc.bih.nic.in/Docs/Home‐
based‐Workers.pdf.
• Thai Health, 12 Health Indicators of Thailand’s Workforce: Informal Sector, 2010.
• UN Women and Baidari ILO, “Report on Experience Sharing and Advocacy Workshop: Integrated Support Programme to Home Based Workers,” Book,
April 15, 2011, http://www.ilo.org/islamabad/whatwedo/publications/WCMS_155223/lang‐‐en/index.htm.
• The World Bank. (2013). World Development Indicators: Labor Force ‐ total [Data file]. Retrieved from
http://data.worldbank.org/indicator/SL.TLF.TOTL.IN.](https://image.slidesharecdn.com/37442dc9-fd4a-4fbb-b460-904888b88f57-external-150309101532-conversion-gate01/85/Health-Vulnerabilities-of-Informal-Workers-108-320.jpg)




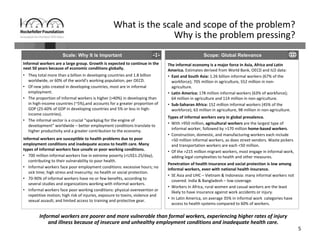
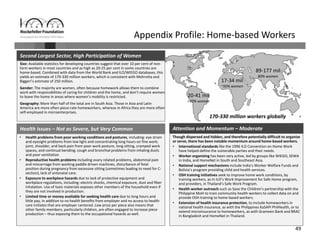
Informal workers face significant health risks due to employment insecurity and lack of access to affordable healthcare. They number over 1.8 billion worldwide, or 60% of the global workforce. Informal workers experience higher rates of illness and injury because their jobs often involve unsafe conditions and provide little social protection. While some countries and organizations have begun programs to expand healthcare access and coverage, informal workers remain a highly vulnerable population given the diversity of their needs and lack of systematic data about their health and employment conditions.








































































































