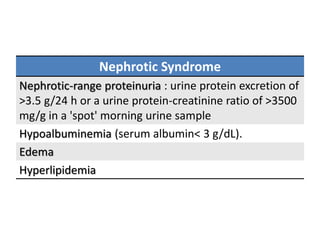
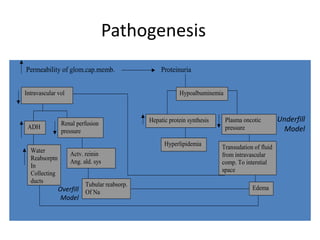
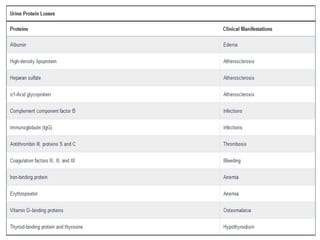
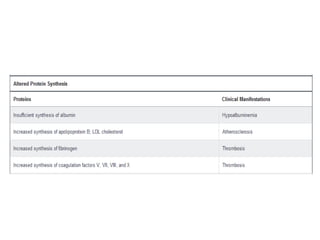
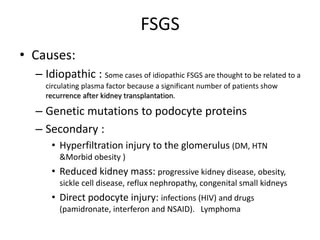
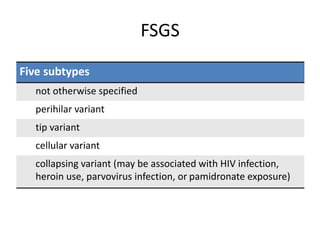
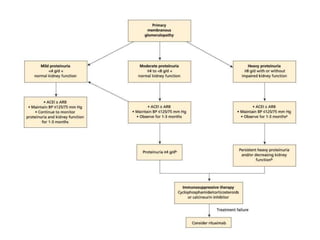
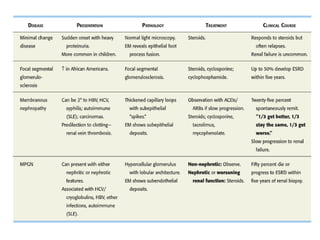
Nephrotic syndrome is characterized by proteinuria, hypoalbuminemia, edema, and hyperlipidemia. It can be caused by primary glomerular diseases like minimal change disease, membranous nephropathy, and focal segmental glomerulosclerosis or secondary to conditions like diabetes, infections, drugs, and amyloidosis. Treatment involves managing edema, lipids, and the underlying cause. Kidney biopsy is needed to identify the specific glomerular lesion causing nephrotic syndrome and guide treatment.