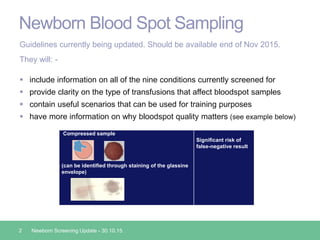
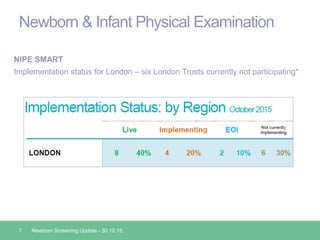
Public Health England is responsible for quality assuring the NHS newborn screening programmes. An update was provided on changes to the newborn blood spot and hearing screening guidelines and standards, as well as the implementation of new screening technologies like pulse oximetry screening and the NIPE SMART system for standardized newborn physical examinations. Trusts are encouraged to discuss any concerns about changes to local screening programs to ensure babies continue receiving complete and timely screening.