
Download to read offline
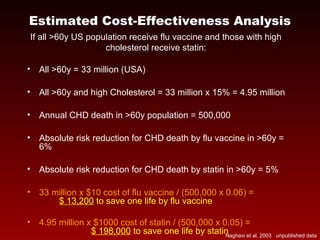

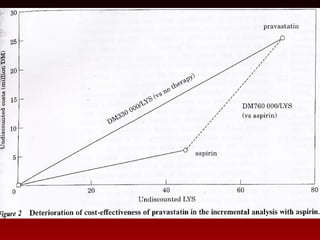
This document summarizes research on the effectiveness and cost-effectiveness of influenza vaccination, statin drugs, and aspirin for preventing cardiovascular events. It finds that influenza vaccination has been shown to reduce hospitalizations for cardiovascular disease by 6-12% and lower mortality by 48-50% based on observational studies. The cost per life saved from influenza vaccination is estimated to be $13,200, much lower than the $198,000 per life saved by statin drugs. The document concludes that influenza vaccination could be a highly cost-effective addition to prevention strategies given its low cost and potential population-level benefits.
























![Csp flu vaccine case presentation - almost final - erik 04072011[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cspfluvaccinecase-presentation-almostfinal-erik040720111-130530202906-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































































