既往歴・アレルギー歴なし。
喫煙10本/日。飲酒24単位/週。
服用中の薬剤なし。
心理学専攻の大学院生。既婚。3歳と4歳の子供と4人暮らし。
There is nosignificant previous medical history or history of
allergy.
He smokes 10 cigarettes per day and drinks 24 units of
alcohol per week.
He is not taking any medication currently.
He is a graduate student doing an MA in psychology.
He lives with his female partner and they have two children
aged 3 and 4 years.
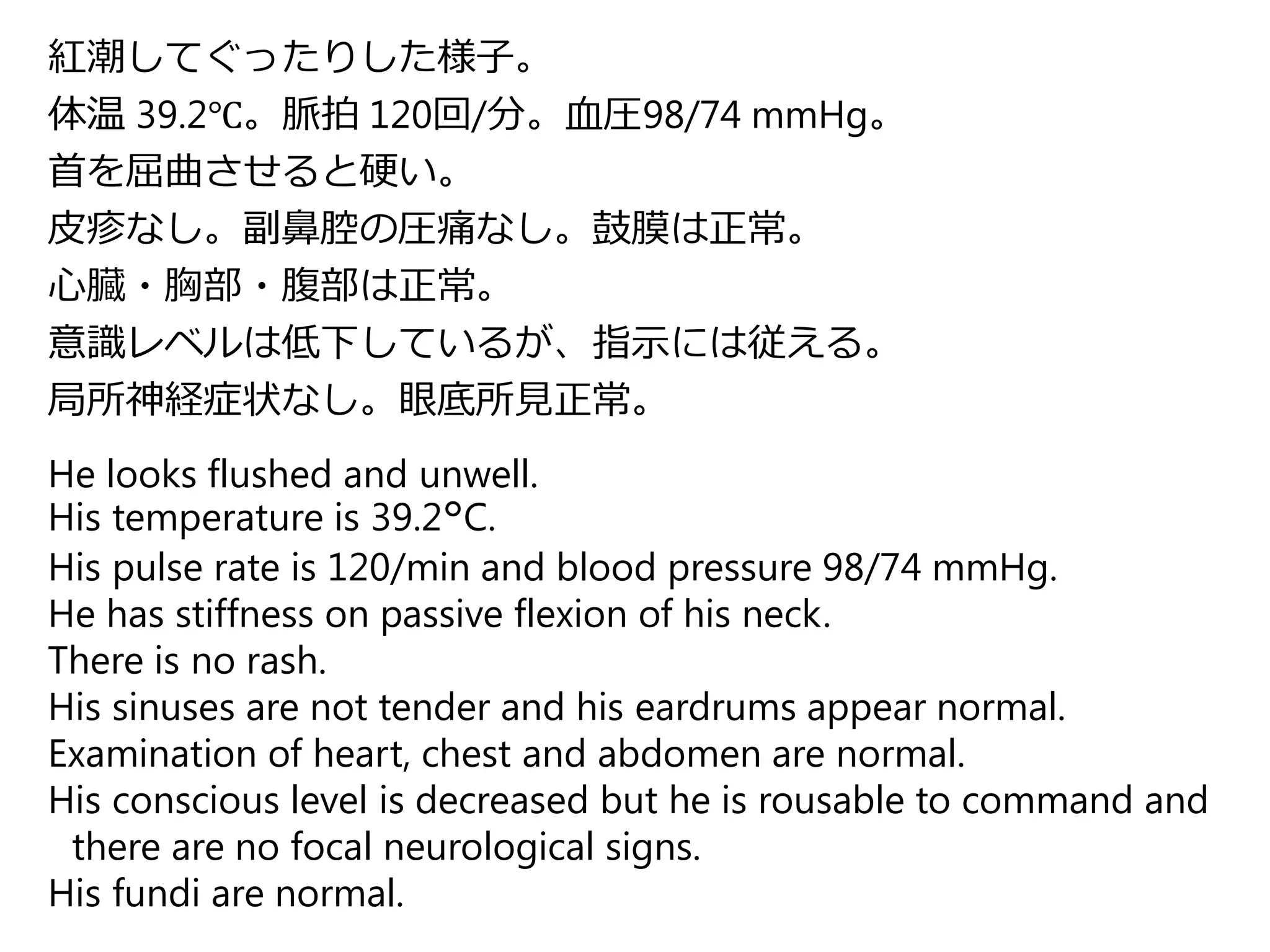
紅潮してぐったりした様子。
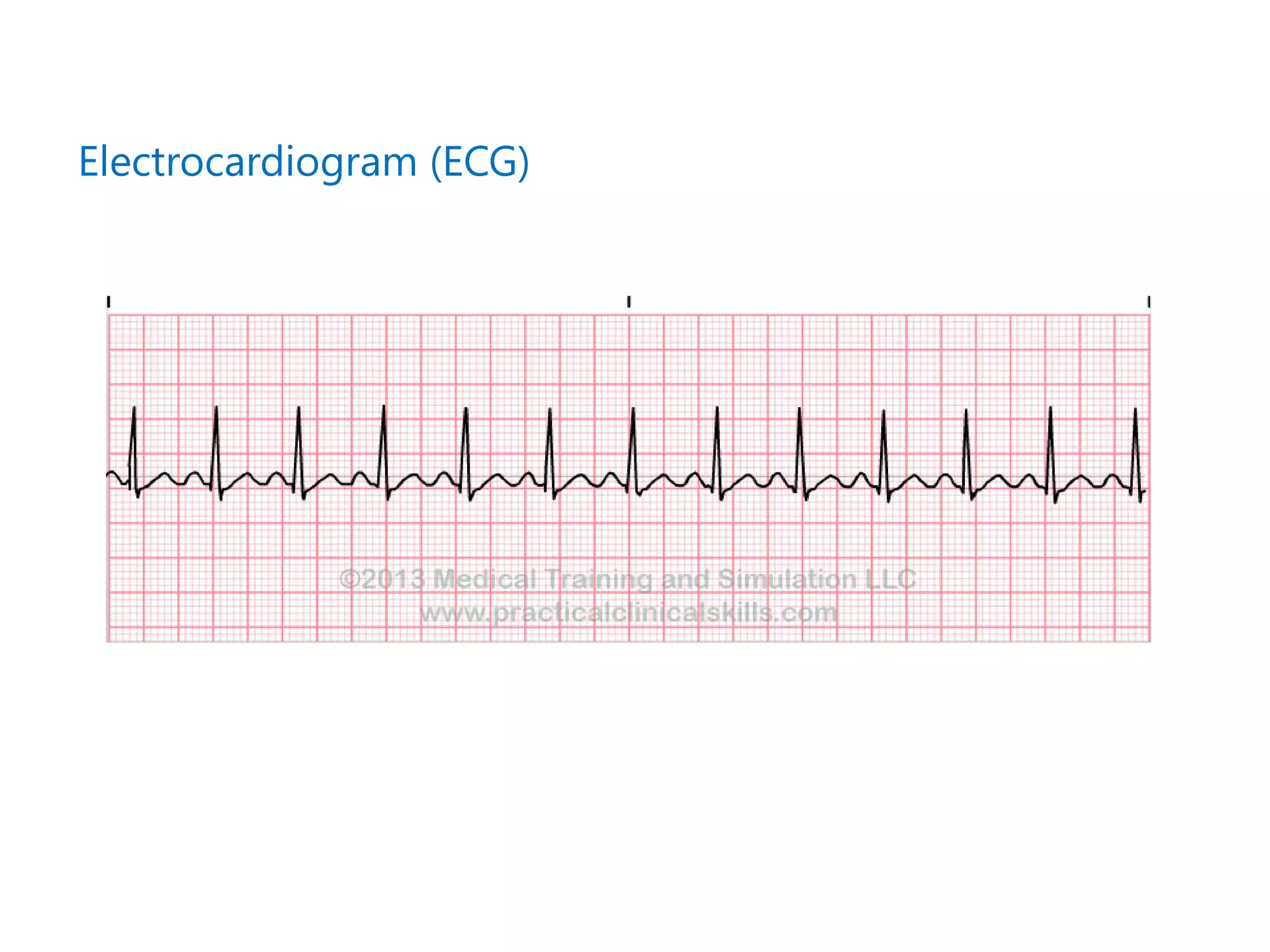
体温 39.2℃。脈拍 120回/分。血圧98/74mmHg。
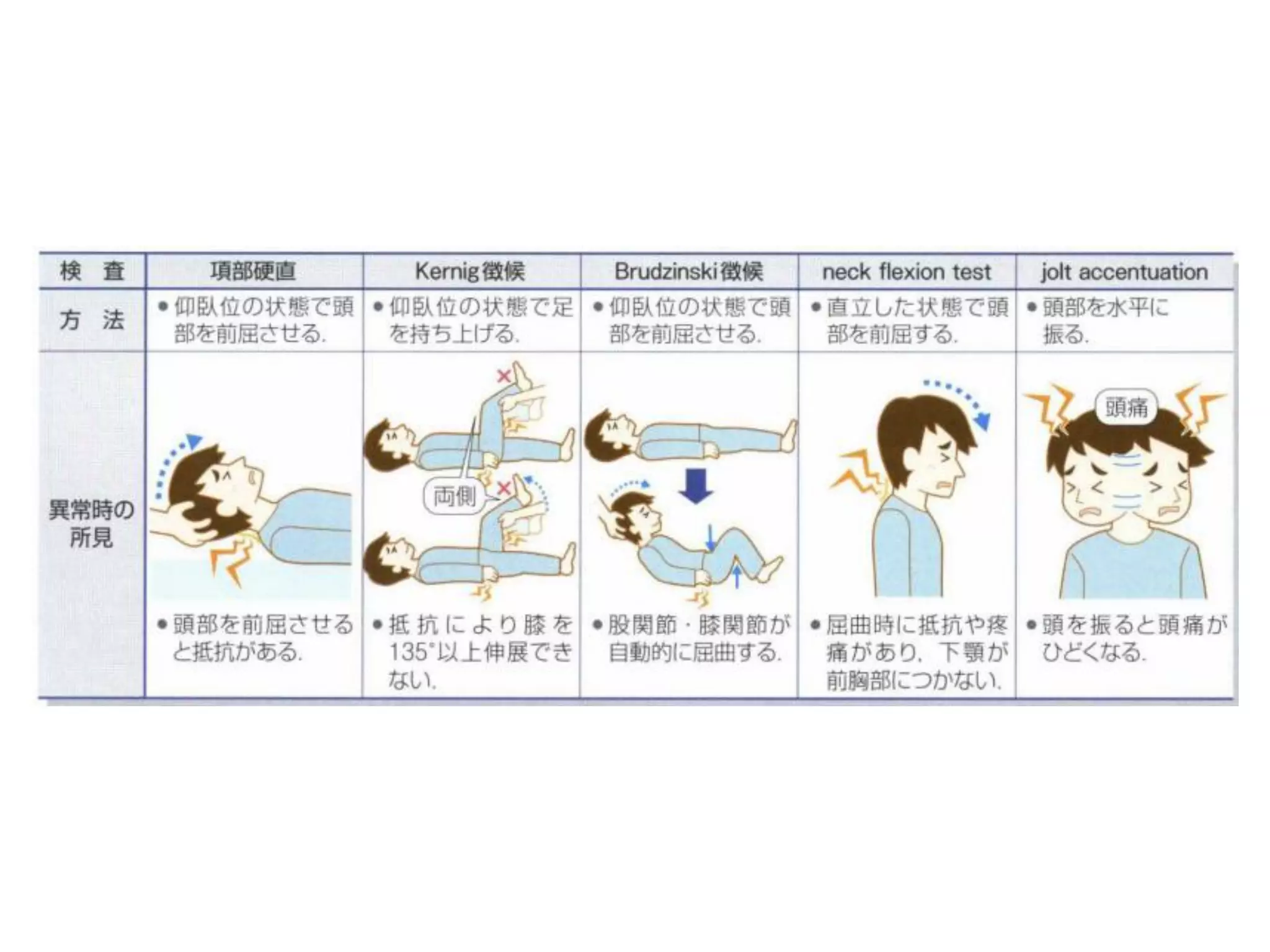
首を屈曲させると硬い。
皮疹なし。副鼻腔の圧痛なし。鼓膜は正常。
心臓・胸部・腹部は正常。
意識レベルは低下しているが、指示には従える。
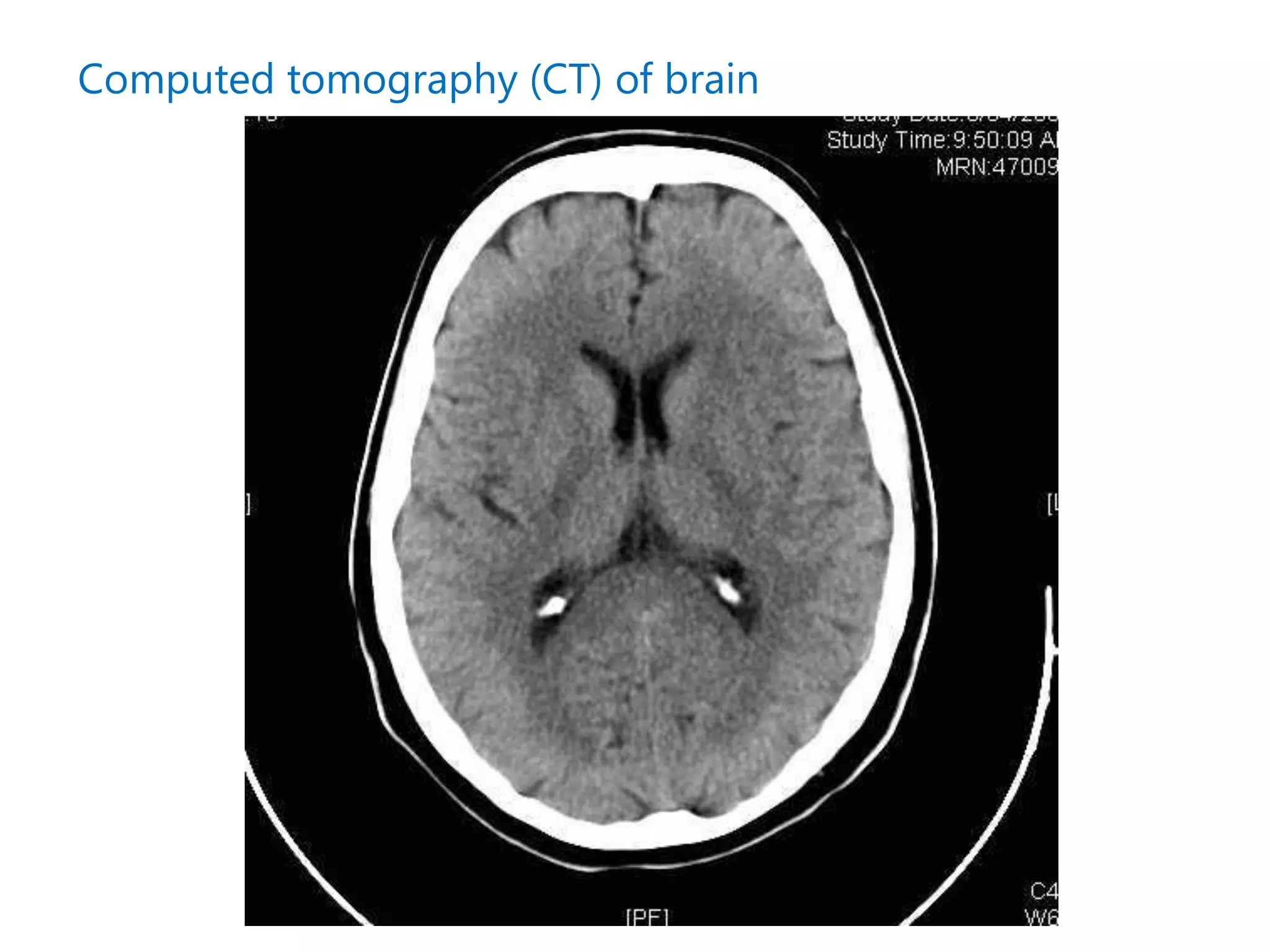
局所神経症状なし。眼底所見正常。
He looks flushed and unwell.
His temperature is 39.2°C.
His pulse rate is 120/min and blood pressure 98/74 mmHg.
He has stiffness on passive flexion of his neck.
There is no rash.
His sinuses are not tender and his eardrums appear normal.
Examination of heart, chest and abdomen are normal.
His conscious level is decreased but he is rousable to command and
there are no focal neurological signs.
His fundi are normal.






















![[2年生] 熊本県の地域医療の現状・原因・対策](https://cdn.slidesharecdn.com/ss_thumbnails/2-131119231710-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






























