Download to read offline







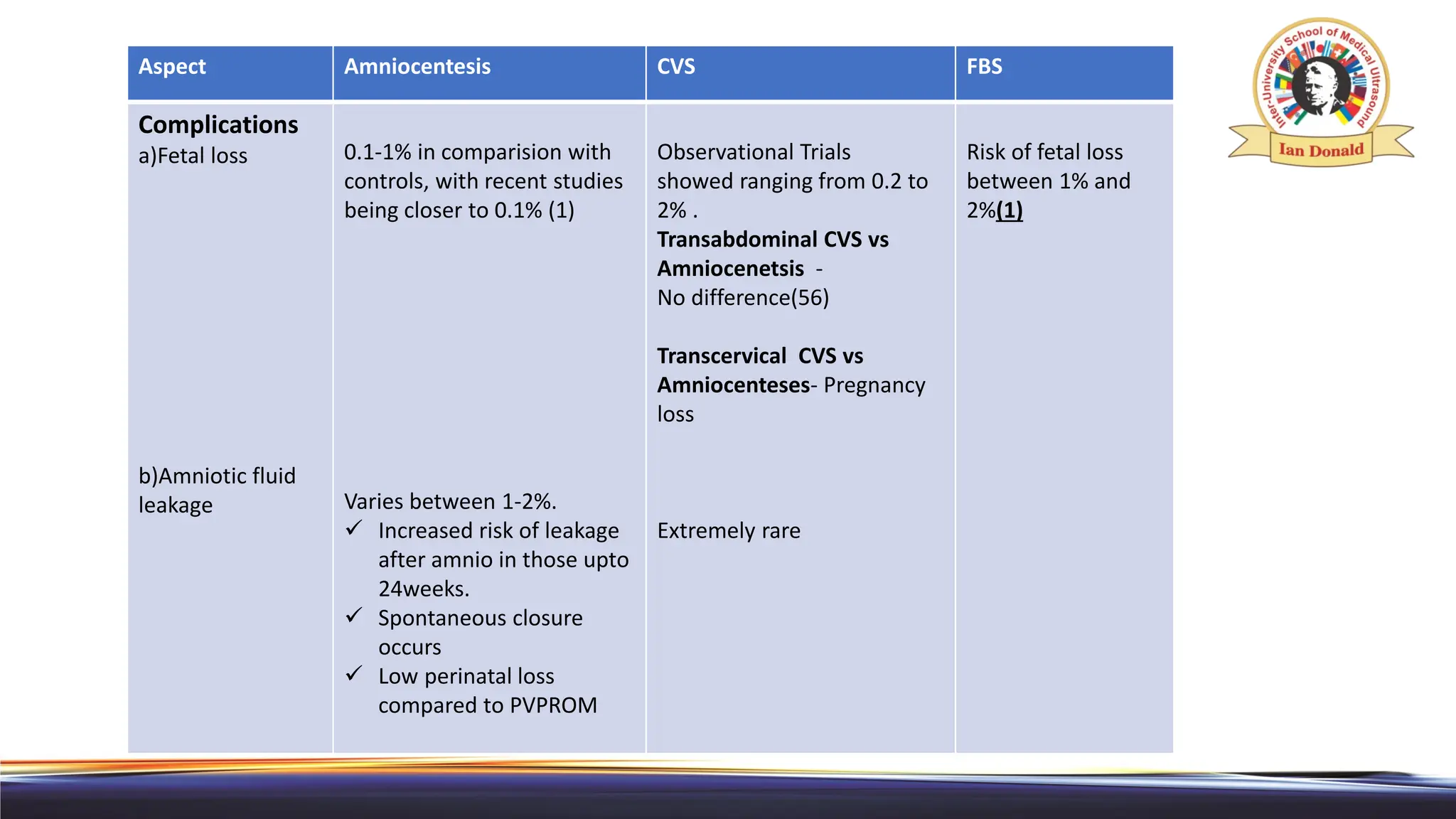









This document discusses invasive prenatal diagnostic tests including cordocentesis, amniocentesis, and chorionic villus sampling. It provides details on the prerequisites, techniques, risks, and post-procedure care for each test. Cordocentesis involves puncturing the umbilical vein under ultrasound guidance to obtain a fetal blood sample and has a risk of fetal loss between 1-2%. Amniocentesis involves inserting a needle through the abdomen into the amniotic sac to extract amniotic fluid and has a risk of fetal loss up to 1%. Chorionic villus sampling collects placental tissue and has a fetal loss risk of 1-2%. The document emphasizes aseptic technique and ultrasound guidance for



































































