Downloaded 177 times




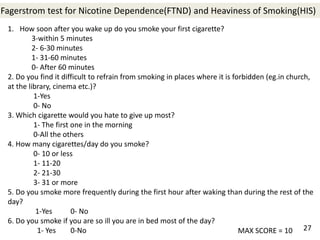
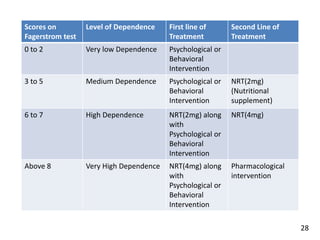

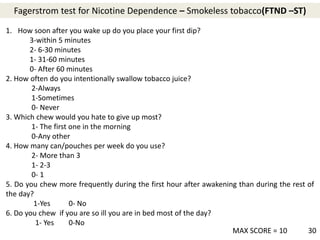
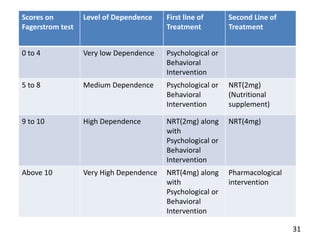
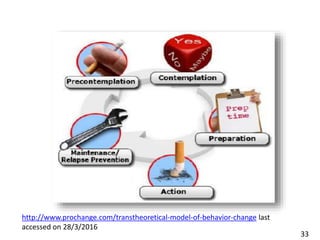
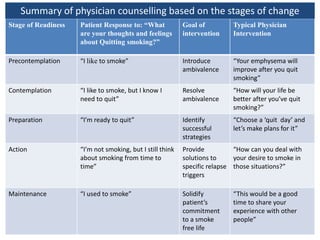




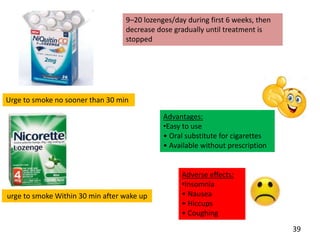
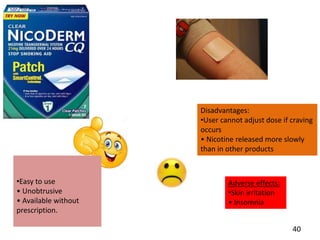
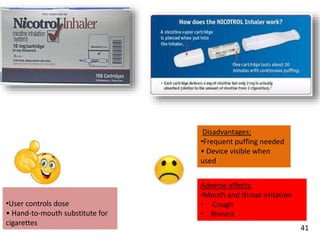



This document provides an overview of a tobacco cessation programme, including: - Details on tobacco production, consumption, and the Global Adult Tobacco Survey. - Scales to measure nicotine dependence like the Fagerstrom test. - Models of behavior change like the Transtheoretical Model. - Approaches to cessation like nicotine replacement therapy, pharmacotherapy, and behavioral counseling. - Studies showing the success of tobacco cessation programs in India, including higher success rates for programs involving hospitals, counseling, and certain drug combinations. - Barriers to cessation like a lack of trained health professionals and knowledge about tobacco's harms.






























































































