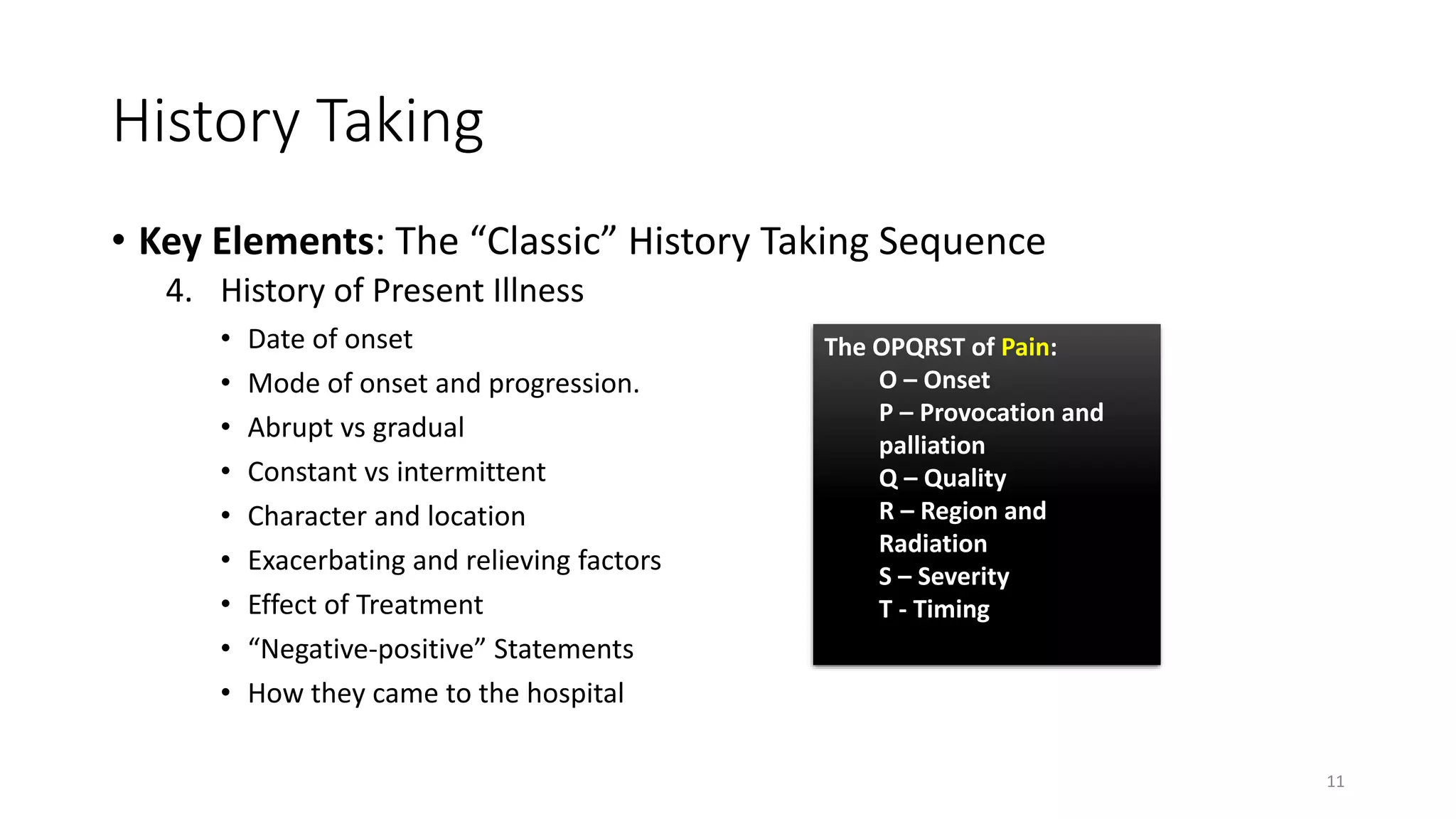
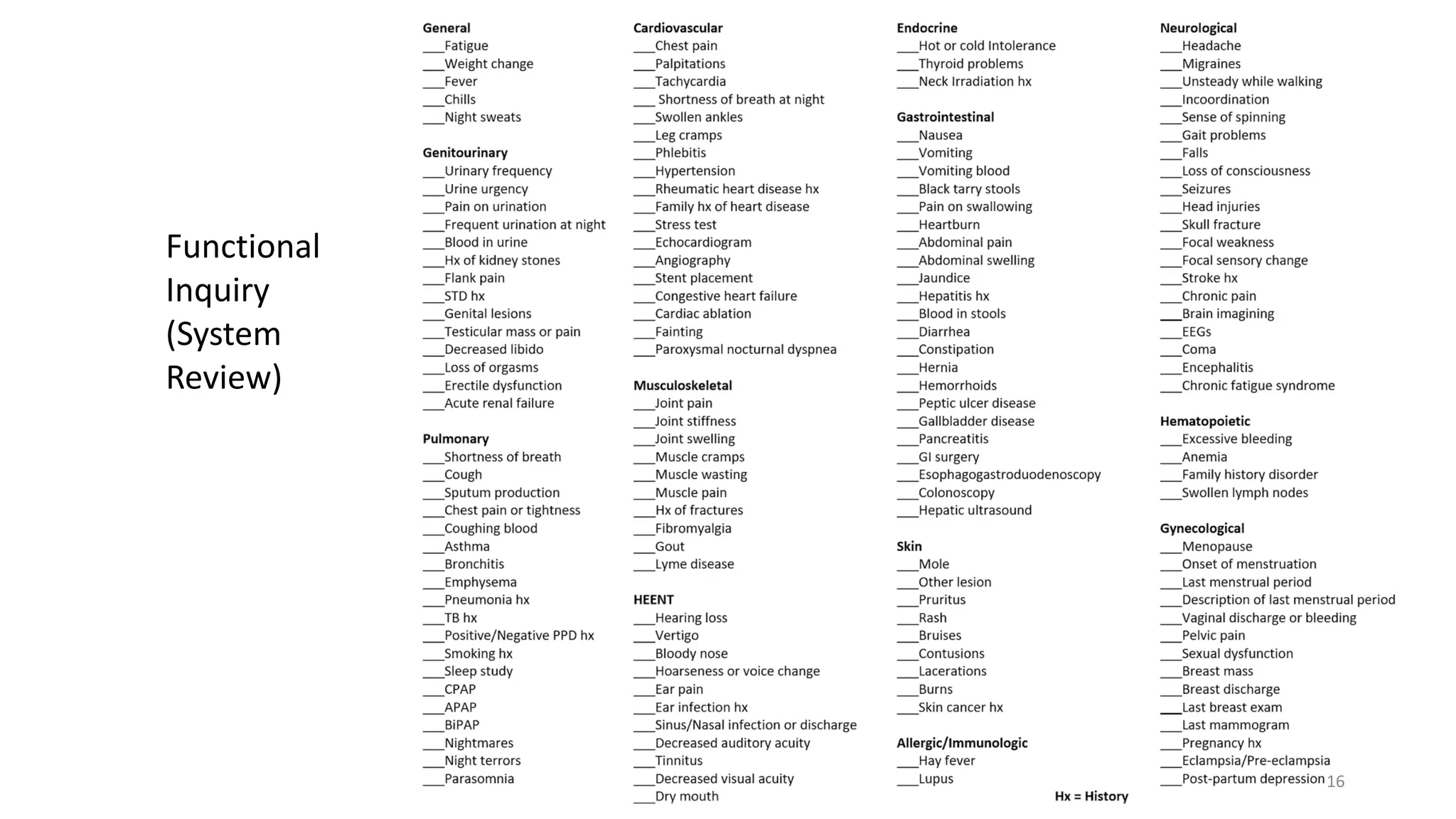
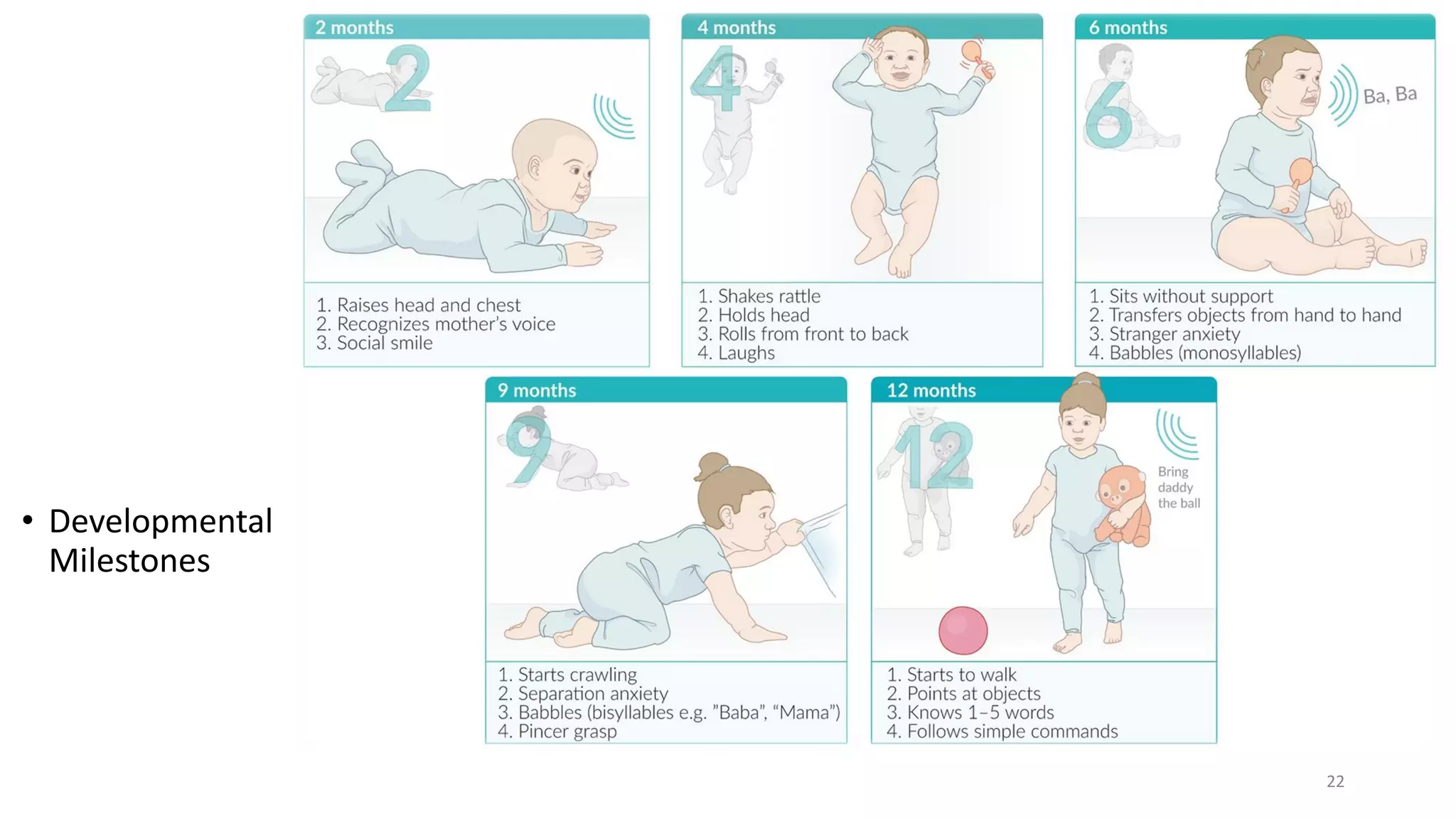
The document outlines the key components of taking a patient's medical history, including establishing rapport, documenting symptoms, and developing a differential diagnosis. It discusses the optimal setting for history taking and reviews the classic sequence, including chief complaints, history of present illness, past medical history, and targeted questions for specific conditions. The goal is to systematically gather a comprehensive history through patient-centered communication to aid in diagnosis and treatment planning.