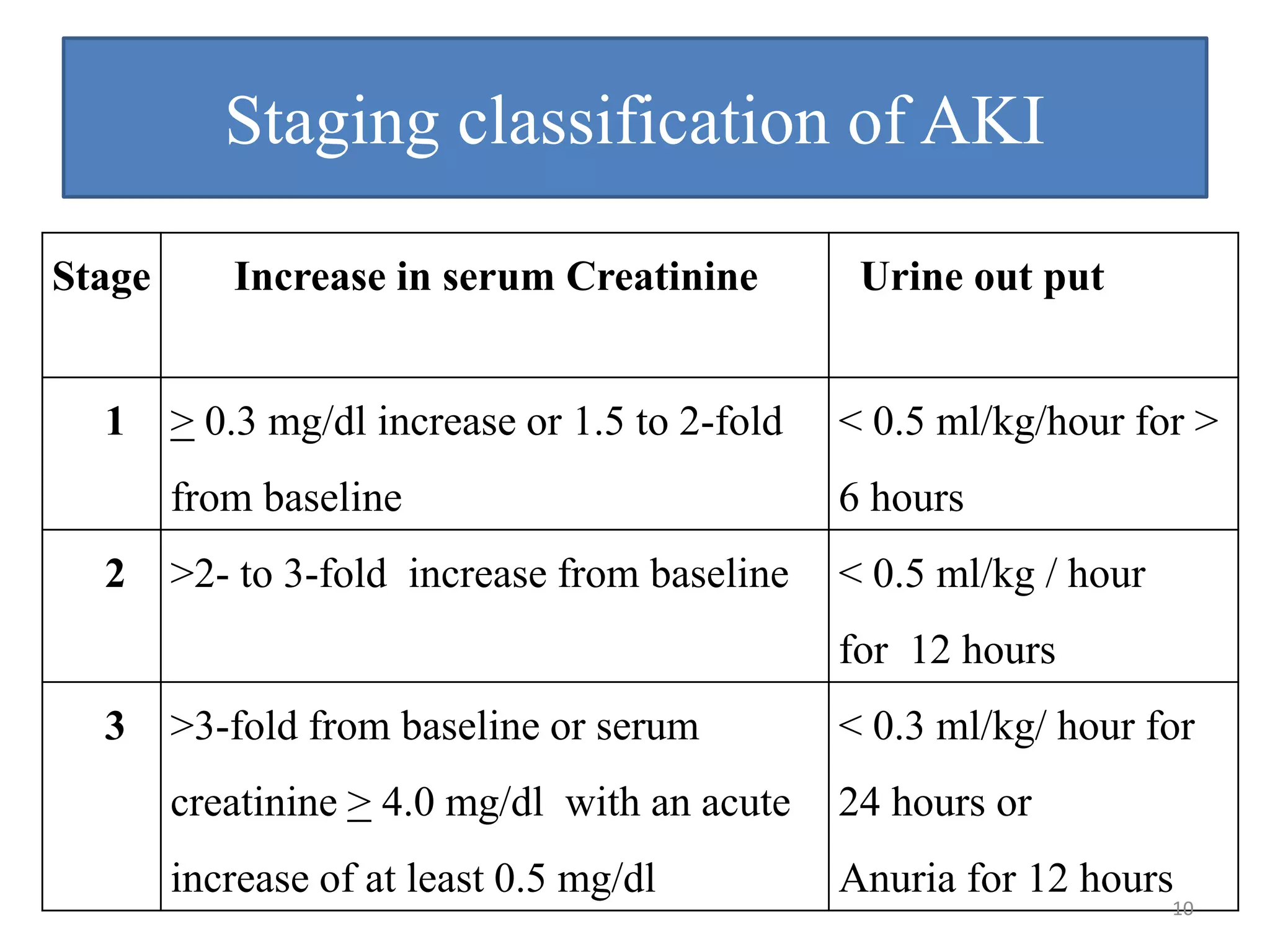
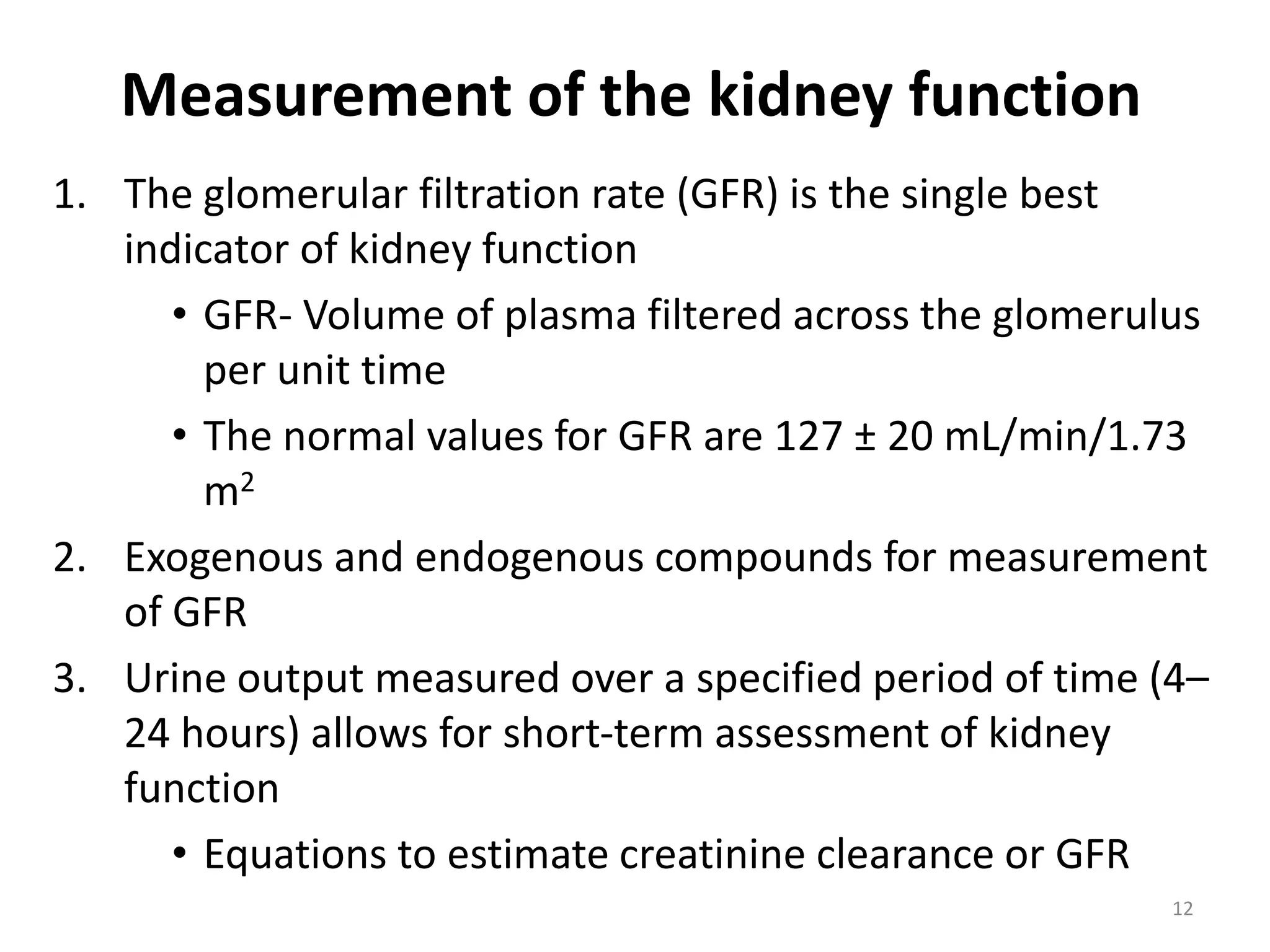
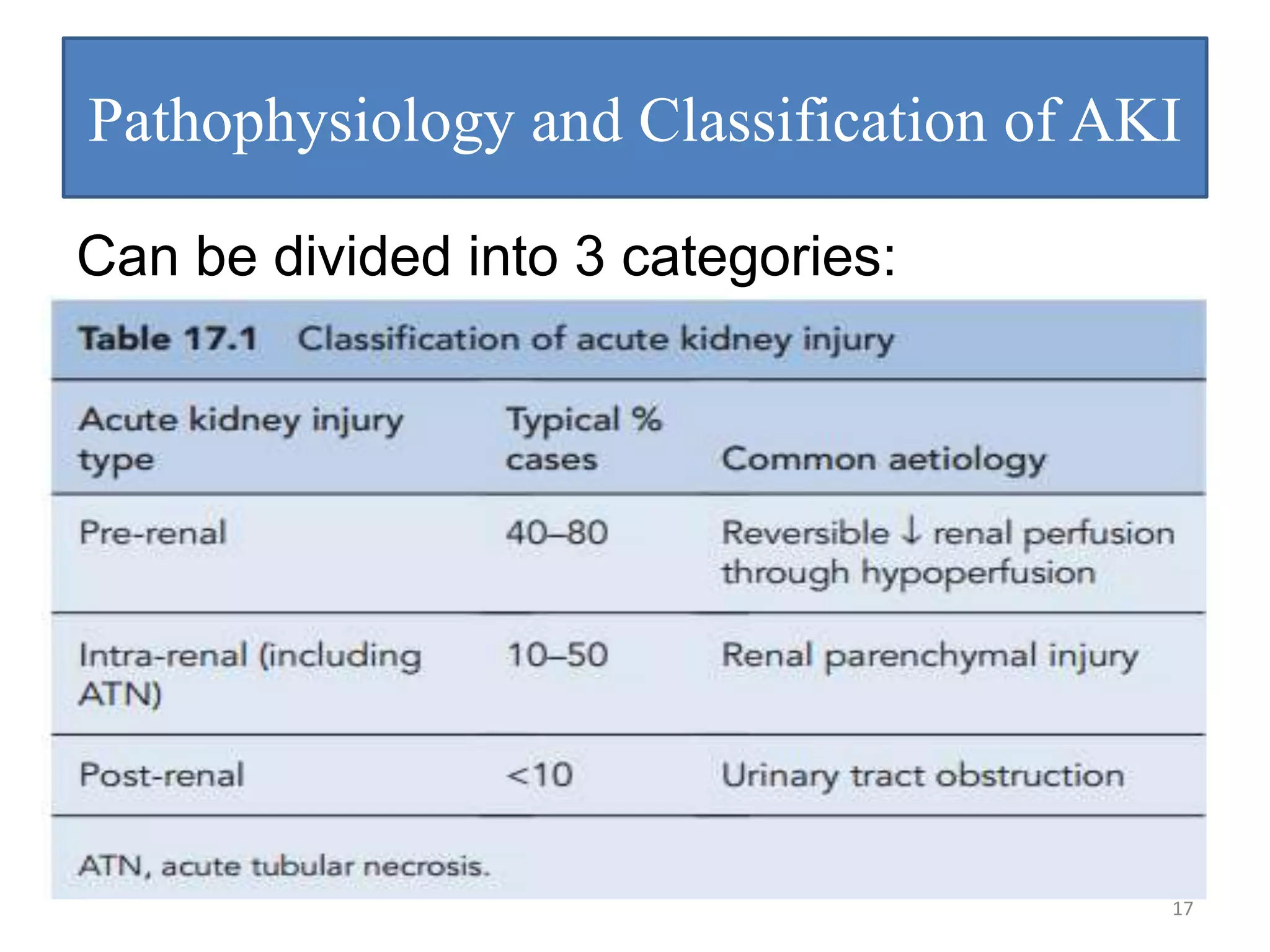
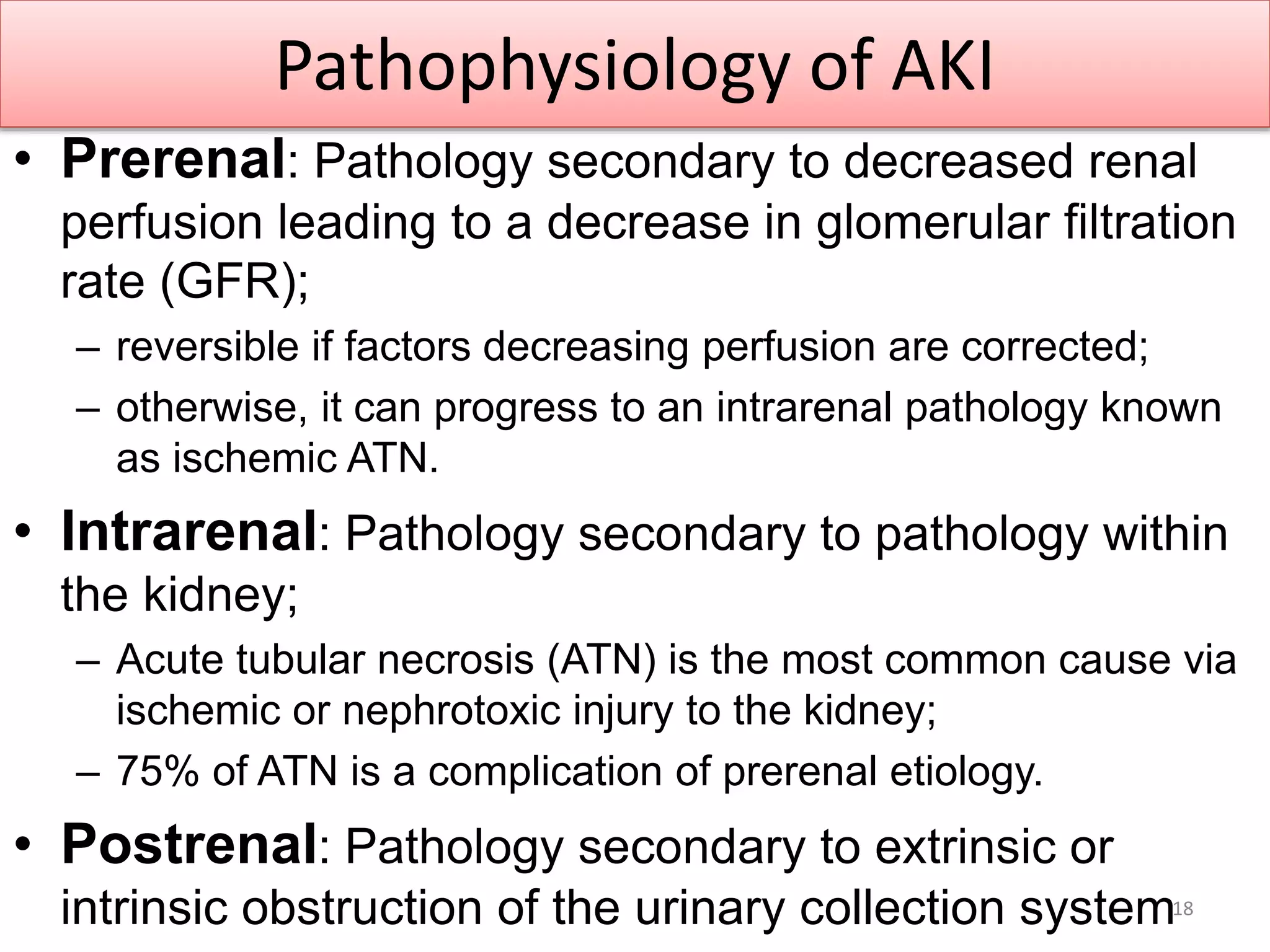
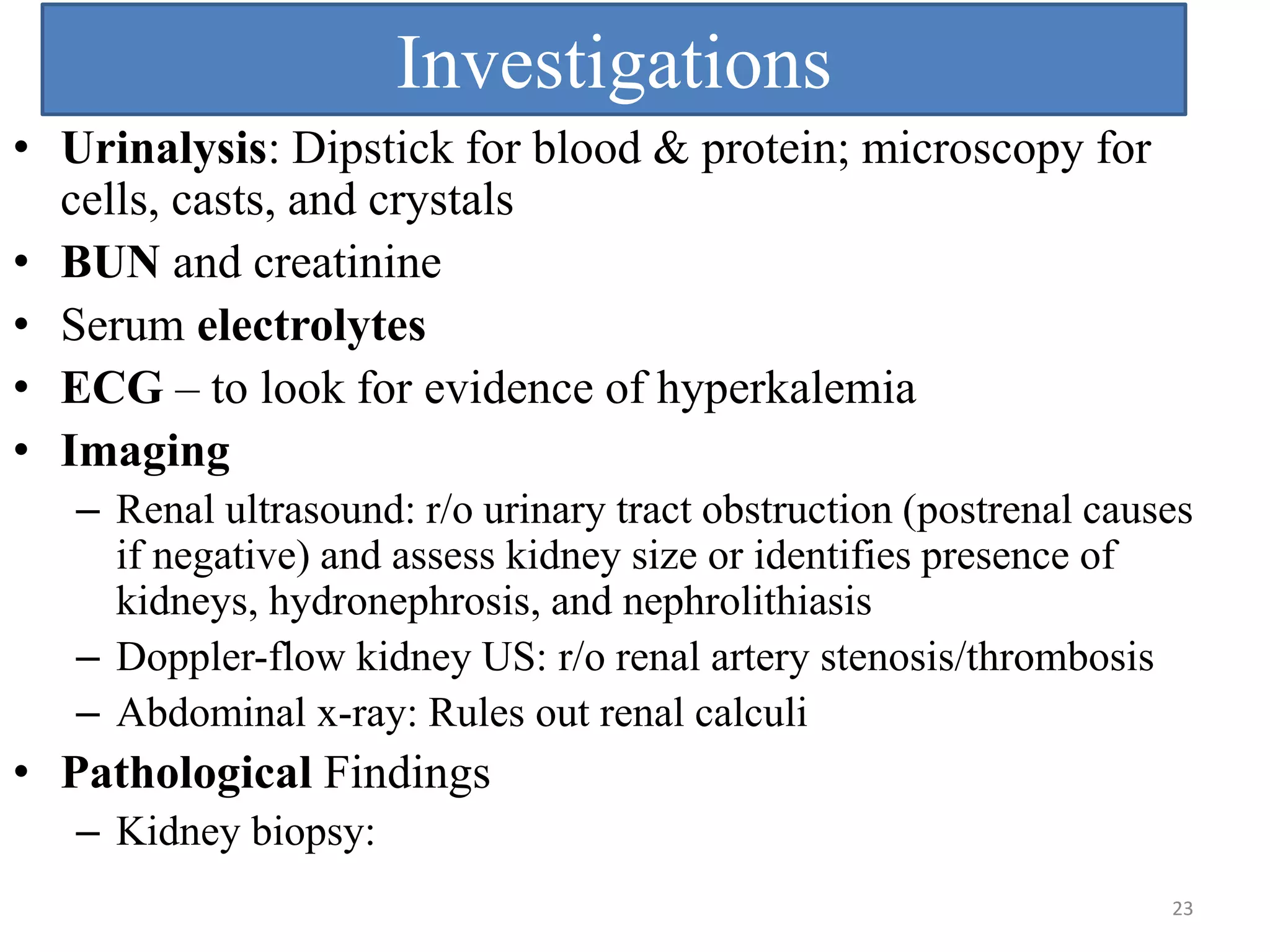
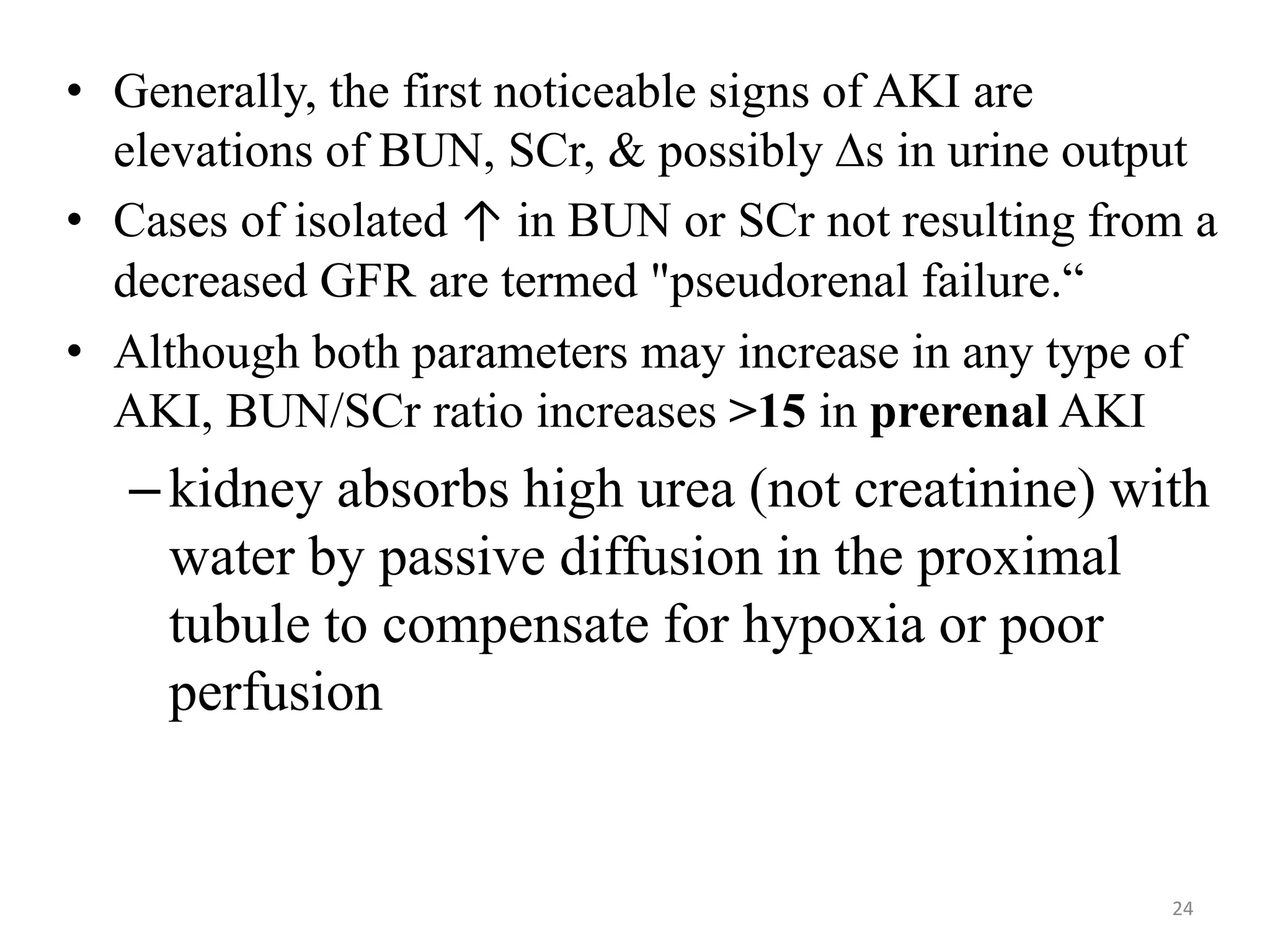
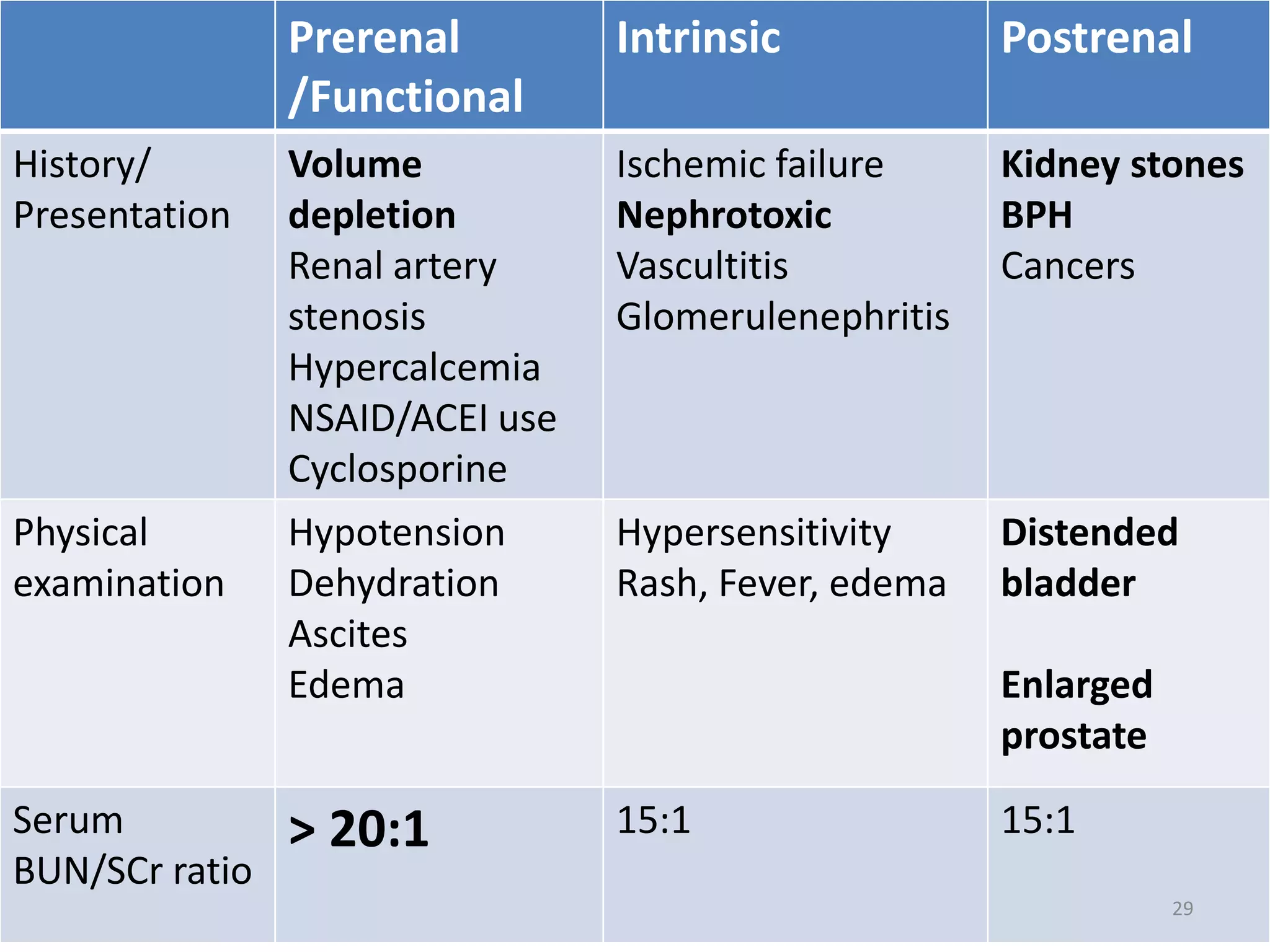
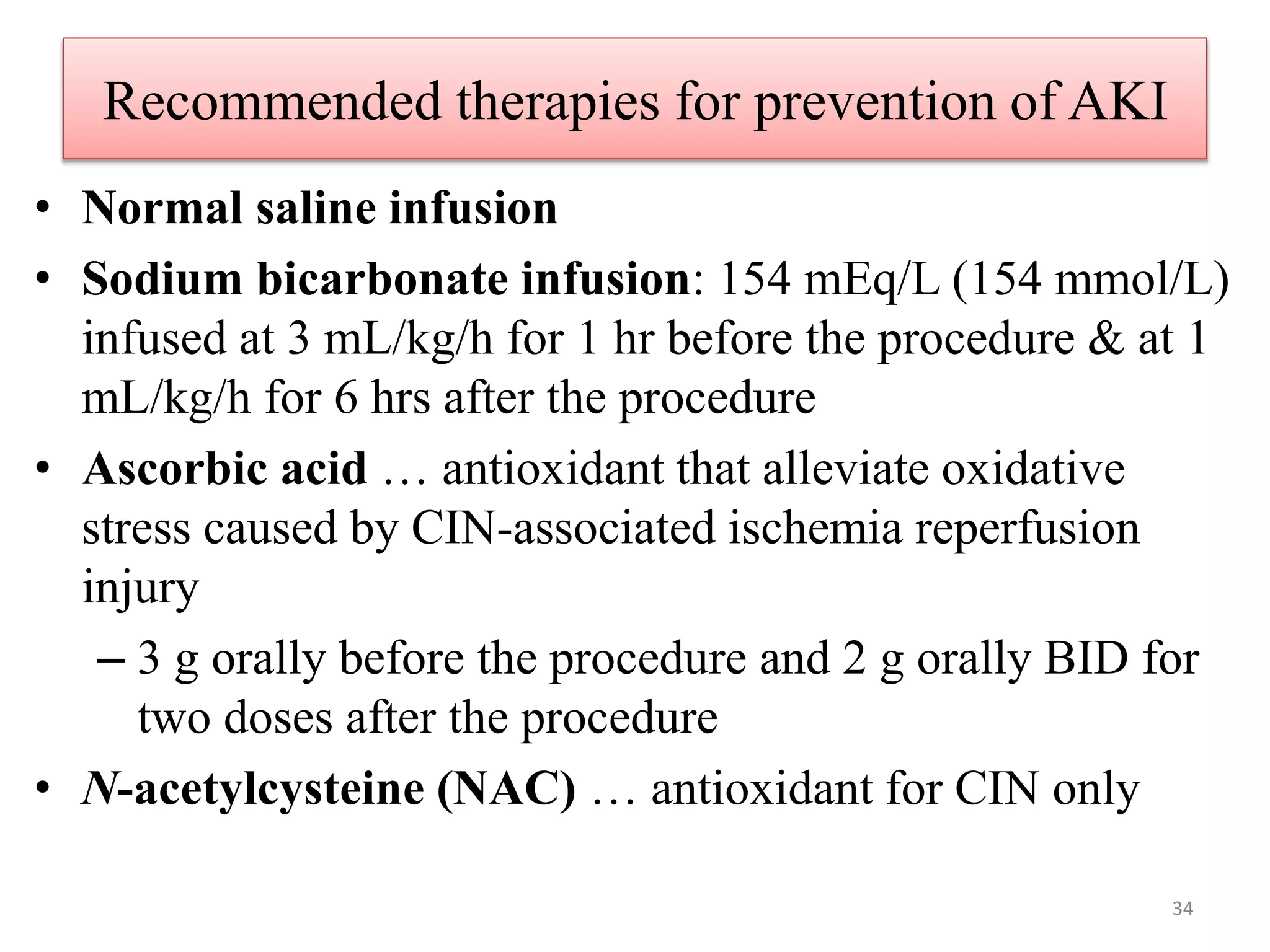
This document provides an overview of pharmacotherapy for renal disorders. It begins by outlining various renal disorders including acute renal failure, chronic renal failure, drug-induced renal disease, glomerulonephritis, nephrotic/nephritic syndromes, acid-base disorders, and disorders of fluid and electrolyte homeostasis. It then focuses on acute kidney injury (AKI), discussing definition, staging, risk factors, pathophysiology, clinical presentation, investigations, and management. Prevention and treatment of specific causes of AKI like contrast-induced nephropathy and nephrolithiasis are also covered.



















![Fractional excretion of Na
• Evaluating the urine sodium concentration and percent
excreted (FeNa) is particularly helpful in differentiating
between a pre-renal AKI and ATN.
• In pre-renal, kidneys should excrete very little Na as a
compensatory mechanism to increase water reabsorption.
• Under normal conditions, the kidneys excrete
approximately 1 to 2% of the total sodium intake (normal
FeNa value).
• * FE Na= [(UNa × SCr)/(SNa × UCr)] × 100
Where U= urine and S=serum
* < 1 prerenal,
>1 renal
26](https://image.slidesharecdn.com/1acutekidneyinjury-230503135240-39a11d10/75/1-Acute-Kidney-Injury-pptx-26-2048.jpg)
![• Urinary Na < 20
• Urine Osms > 500
• Highly concentrated urine (>500 mOsm/kg [>500
mmol/kg]) suggests stimulation of antidiuretic and intact
tubular function.
• These findings are consistent with prerenal
azotemia.
• Common lab abnormalities in ARF:
– Increased: K+, phosphate, Mg, uric acid
– Decreased: Hematocrit (Hct), Na, Ca
27](https://image.slidesharecdn.com/1acutekidneyinjury-230503135240-39a11d10/75/1-Acute-Kidney-Injury-pptx-27-2048.jpg)







![1. Contrast-Induced Nephropathy (CIN)
• Common cause of ATN in inpatients (>0.5 mg/dl ↑ Scr)
• Onset …an ↑in Scr or Oliguria develops w/in 24 hrs
• Prevention:
– N-acetylcystine 600 mg po bid for four doses, with the
first two doses administered prior to contrast exposure
and then the last 2 doses after
– 600 mg PO b.i.d. on day prior to and day of contrast [A]
and
– isotonic NaHCO3 3 mL/kg/h × 1 h before administration
of contrast material and 1 mL/kg/h × 6 h after contrast
material [B].
37](https://image.slidesharecdn.com/1acutekidneyinjury-230503135240-39a11d10/75/1-Acute-Kidney-Injury-pptx-37-2048.jpg)





![Treatment
• Intrinsic: no universal therapy
– Avoid insult
– Consider fluid bolus…..perfusion/urine production
– Loop diuretics for oliguric/euvolemic or hypevolemic
• Furosemide ………..40-80 mg IV every 6-8 hrs or
• Furosemide infusion 40-80 mg IV bolus; then, 10-20 mg/hr iv
• Furosemide is a commonly used intervention.
N.B Studies show that it is ineffective in preventing and treating
ARF [A].
– Dopamine therapy …………1-2 mcg/kg/min….
• Not recommended anymore
– Natriuretic peptides, insulin-like growth factor, and
thyroxine also have no benefit in the treatment of ARF
– Acidosis……………. restrict dietary protein
• HCO3 to maintain arterial pH > 7.35
– Dialysis if needed
43](https://image.slidesharecdn.com/1acutekidneyinjury-230503135240-39a11d10/75/1-Acute-Kidney-Injury-pptx-43-2048.jpg)


![Diet for AKI patients
• Total caloric intake should be 35–50 kcal/kg/d to
avoid catabolism.
• Sodium should be restricted to 2 g/d [A].
• Potassium intake should be restricted to 40
mEq/d.
• Phosphorus should be restricted to 800 mg/d. If it
becomes high, treat with calcium carbonate or
other phosphate binder [A].
• Magnesium compounds should be avoided.
46](https://image.slidesharecdn.com/1acutekidneyinjury-230503135240-39a11d10/75/1-Acute-Kidney-Injury-pptx-46-2048.jpg)































































































