Downloaded 89 times

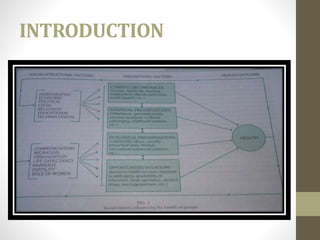







The document provides an extensive overview of sociology's relationship with lifestyle and oral health, discussing key concepts such as community, social structure, and social inequality and their impacts on health. It emphasizes that understanding sociological factors is crucial for effective dental care and public health planning. Additionally, it highlights various social determinants that affect oral health outcomes across different socioeconomic classes.


































![Unit_1._Introduction_to_Sociology_[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/unit1-240821164119-baffadf4-thumbnail.jpg?width=640&height=640&fit=bounds)









































