Downloaded 21 times


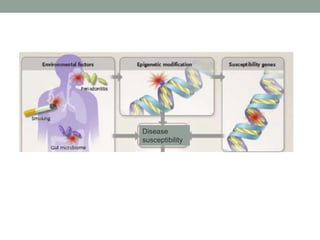
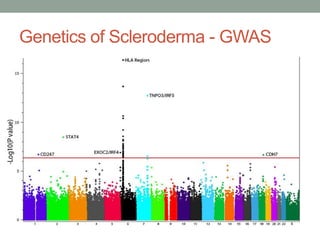
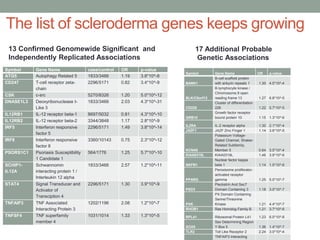

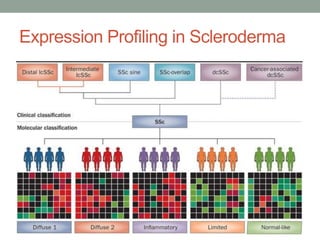


The document discusses the evolution and significance of genomic research, particularly highlighting the advancement of the Human Genome Project and its implications for understanding human disease, particularly scleroderma. It details the genetic associations found in scleroderma and the complexity of its genetics, including the influence of multiple genes and environmental factors on disease susceptibility. Additionally, it explores the potential of personalized medicine to tailor treatments based on individual genetic makeup, while also addressing the challenges faced in interpreting genomic data and implementing personalized approaches in clinical settings.