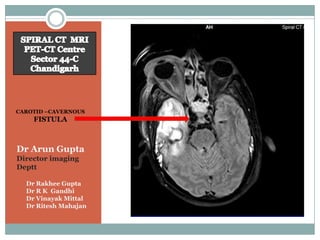
1. CAROTID –CAVERNOUS
FISTULA
Dr Arun Gupta
Director imaging
Deptt
Dr Rakhee Gupta
Dr R K Gandhi
Dr Vinayak Mittal
Dr Ritesh Mahajan
2. CAROTID CAVERNOUS
FISTULA
DEFINITION BEST DIAGNOSTIC CLUE
Carotid – cavernous Proptosis .
fistula ( CCF ), Direct CCF,
Dilated superior
High velocity CCF .
ophthalmic vein and
High flow fistula between
Cavernous sinus .
the cavernous ICA and
cavernous sinus .
3. CAROTID CAVERNOUS
FISTULA
CT FINDINGS MR FINDINGS
Large cavernous sinus with
Proptosis signal voids ( t1w) .
Orbital edema TI ( C) :
Enlarged extra ocular Enlarged enhancing cavernous
sinus and SOV.
muscles Adjacent or diffuse dural
enhancement .
SAH : secondary to reflux
MRA :
from the cortical veins Increased flow related signal in
( Rupture ) . the CS .
Increased signal void in CS : Due
Prominent SOV and to increased turbulence
Cavernous sinus Flow in SOV and /or trans-sellar
( may be bilateral) . collaterals .
4. CAROTID CAVERNOUS
FISTULA
USG findings Angiographic findings
Very rapid filling of enlarged
Doppler shows reversal CS after ICA injection .
of the flow direction in Common drainage pathways
SOV ( posterior to ( SOV & IOV ..Facial vein) .
Other drainage pathways
anterior ) . Superior and inferior petrosal
sinuses ..INTERNAL JUGULAR
VEIN
Opposite CS via trans-sellar or
basilar plexus .
Vein of Rosenthal ..vein of Galen .
Signs of danger : Filling of cortical
veins , pseudoaneurysm , CS
varices , thrombosis / obstruction
of venous drainage .
5. D/D
Enlarged Extra ocular
Enlarged SOV
muscles
CS thrombosis : No Grave’s and
fistula on angiography . inflammatory
Grave’s disease : Signs pseudotumor
of hyperthyroidism. Intra-muscular masses
Masses in orbital apex. ( Metastases) .
6. CAROTID CAVERNOUS
FISTULA
Pathology Etiology & types
Skull base fracture commonest .
Blood from cavernous Ruptured cavernous ICA aneurysm .
ICA to CS ..SOV and Younger individuals (prone to trauma )
average age ( 37 years) . Gender : male .
petrosal sinuses.
Individual with collagen vascular
Reflux from cerebral disorders
cortical veins occurs Most tears involve the proximal
horizontal or vertical cavernous ICA .
when SOV/IOV and
Type A : Direct communication
petrosal sinuses cannot between ICA and cavernous sinus
handle large blood Type B-D : Indirect
volume …increased risk communications between the
of SAH . meningeal/dural branches of
ICA/ECA and cavernous sinus .
7. PROMINENT
SUPERIOR OPTHALMIC VEIN
T1W SEQUENCE T2W SEQUENCE
11. CAROTID CAVERNOUS
FISTULA
PRESENTATION TREATMENT
Symptoms develop either Spontaneous thrombosis
spontaneously or days / rare , progresses if
wks after trauma untreated .
Bruit ( 50%) , pulsating
ICA / JUGULAR vein
exophthalmos , orbital
edema / erythema , compression ..only for
decrease vision, glaucoma , small CCF
headache . Severe rapid Embolization (coiling or
vision loss ,SAH , Focal
deficits ( CN 3-6). ( these balloon) : Trans-arterial
findings may be unilateral or transvenous .
/ bilateral) . Surgery / Gamma knife .
12. References
•F A T T A H I T T E T A L : T R A U M A T I C C A R O T I D - C A V E R N O U S
FISTULA ; PATHOPHYSIOLOGY AND TREATMENT . J
CRANIOFACSURG 14 :240-46,2003.
•C H U M A N H E T A L ; S P O N T A N E O U S D I R E C T C A R O T I D -
CAVERNOUS FISTULA IN EHLER-DANLOS SYNDROME
TYPE 4 : TWO CASE REPORTS AND A REVIEW OF THE
LITRETURE . J NEUROOPHTHALMOL 22:75-81,2002.
•D I A G N O S T I C I M A G I N G B R A I N O S B O R N