
Downloaded 24 times
![The URC proposed framework for its
Communication Intervention Cycle Towards
Social Mobilization (Bandalaria, 2017)
Bandalaria, M. (2017). Module 6 Guide [COMM 380 Class handout]. University of the
Philippines Open University](https://image.slidesharecdn.com/380acsmimplementationstrategies-170504140941/85/ACSM-Implementation-Strategies-7-320.jpg)
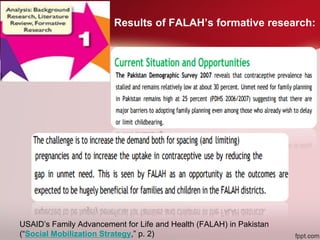
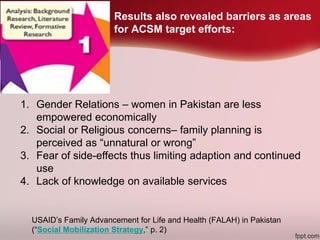
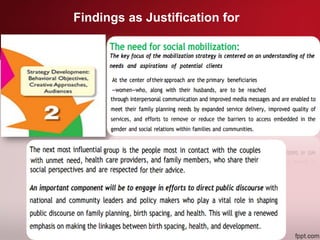

The document outlines various strategies for implementing advocacy and social mobilization programs, with a focus on the USAID's Family Advancement for Life and Health (FALAH) framework in Pakistan. It details the necessity of formative research to identify barriers and opportunities while emphasizing collaboration between political, community, and governmental entities to enhance social mobilization efforts. Additionally, it proposes a set of 15 steps aimed at fostering behavior change to support these initiatives.































































