1. When does one suspect P ?
Can one clinically differentiate between bacterial and viral
etiology in OPD setting?
How does one confirm the diagnosis?
•
•
4
4
4
4
•
4
4
. .
•
haryngo-tonsillitis
Acute Pharyngitis : Acute pharyngitis is an inflammatory syndrome involving the
pharynx and/or tonsils resulting in fever, sore throat, foul breath and pharyngeal
erythema/exudates. It may have only nasal symptoms (Nasopharyngitis, usually
due to rhinovirus) or may be without any significant nasal symptoms
(Tonsillo-pharyngitis, could be bacterial or viral).
Acute Tonsillitis : Patients have a fever, sore throat, foul breath, dysphagia
(difficulty swallowing), odynophagia (painful swallowing), and tender cervical lymph
nodes.
Possible differentiating points between viral and bacterial Pharyngo-tonsillitis are
discussed in the Table on the opposite page. There is a considerable overlap
between the symptoms and clinical differentiation is difficult
More the qualifying features in a category, more are the chances of
getting the etiology correct. Absence of throat pain or tender adenopathy or
pharyngeal erythema has high negative predictive value for bacterial Pharyngo-
tonsillitis while their positive predictive value is only 45-50%.
Blood count, ESR and C-reactive protein level can help, but have a low
predictive value.
Throat culture is considered the gold standard for diagnosing streptococcal
pharyngitis.
A positive result does not reliably distinguish acute streptococcal pharyngitis
from asymptomatic carriage.
The false-negative rate for a properly performed throat culture is 5-10%, and
many patients with this result are thought to be chronic Group A
Streptococcus (GABHS) carriers, any way not needing treatment. Therefore, a
negative throat culture result has a very high negative predictive value for
GABHS pharyngitis.
The major drawback of throat culture is the 18-48 hours required for results.
This delay does not decrease the ability to prevent rheumatic fever, but it needs
convincing the patients or their caregivers about withholding antibiotics.
Rapid antigen detection tests:
RADTs detect the presence of the Lancefield group A carbohydrate antigen.
Reported sensitivities of RADTs is 65-91% and specificities range between 62-
97%. The enzyme immunoassay tests are better than the latex agglutination
based test The approximate cost for RADT is Rs. 250
Streptococcal antibody testing has no role in the diagnosis of acute
streptococcal pharyngitis as it takes several weeks to become positive. Elevated
titers for both anti-streptolysin-O (ASO) and anti-deoxyribonuclease B (anti-
DNase B) can persist for several weeks, even months.
but should be
attempted.
11
Pharyngo-tonsillitis
1
ACT
Pharyngo-tonsillitis
Definition
•
•
Etiology
•
•
Pharyngitis : Acute pharyngitis is an inflammatory condition of the pharynx and/or
tonsils caused by several different groups of microorganisms.
a. Nasopharyngitis : if only nasal symptoms are present (mostly viral, rhinovirus)
b. Tonsillophryngitis : if present without nasal symptoms (mostly bacterial, can be viral)
Tonsillitis : Tonsillitis refers to inflammation of the pharyngeal tonsils.
Viral cause : Rhino virus (60%), Adenovirus, Enterovirus, Influenza virus, Parainfluenza
virus, etc.
Bacterial cause : Group A ß-hemolytic Streptococci (commonest,15-30% in <3 years
old) Others are, Hemophilus influenzae, Streptococcus pyogenes, N. meningitides,
C. diphtheriae, N. gonorrhea. Mycoplasma pneumoniae involve mostly adolescents.
Pneumococcus, Staphylococcus aureus, are also implicated.
Differentiation between the bacterial and viral infection
10
1
FACTS
Key Messages
•
•
•
•
•
•
•
Pharyngo-tonsillitis is a frequent infection in children.
A large proportion of these cases are viral in nature
The differentiation between a viral and bacterial etiology on clinical grounds is not foolproof, but
this differentiation should be attempted.
Rapid antigen and a throat swab culture are recommended when laboratory testing is necessary.
Bacterial causes should be diagnosed and treated properly to prevent rheumatic fever.
Appropriate treatment should be given even if there is a delay in diagnosis.
Dangerous differentials like diphtheria must be considered in appropriate clinical settings.
Section
I
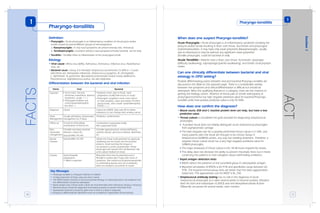
Points Viral Bacterial
Suspicion
Diagnosis Clinical
Initial
Management
Usually self limiting. Symptomatic
management for 3-4days
Follow up To look for Otitis Media,
exacerbation of Asthma etc.
Consider secondary bacterial
infection, culture etc.
Caveats Avoid Ampicillin
preparations
if IMN is suspected
Exclude IMN, HV, HIV
Special
mention
Exclude IMN, HV, HIV
Non-
responders
management
•
•
Acute onset, red eyes,
rhinorrhea, exanthema, diarrhea,
hoarseness, cough +++
Pharyngeal exudates and
cervical lymphadenopathy
less often +
Culture for GABHS. May wait 48 hrs before
antibiotics/ or start therapy after sending culture
Antibiotics, symptomatics
Consider agranulocytosis, immunodeficiency,
systemic disease, gonococcal disease, diphtheria,
etc.
Rheumatic fever may be prevented even if
Penicillin is started upto 9 days after onset of
symptoms. Post-streptococcal glomerulonephritis
is a self-limiting disease and use of antibiotics
does not change its occurrence or course.
Obtain the throat swab specimen by vigorously
swabbing both the tonsils and the posterior
pharynx. Avoid touching the tongue or
oro-pharynx to avoid contamination. Sheep
blood agar with special 0.04 unit Bacitracin disk
is the culture medium of choice.
•
•
toxicity
Explosive onset; pain in throat; rapid
progression;usually little coryza or cough.
Pharyngeal congestion more; more chance
of thick exudates, ulcers and vesicles; Purulent,
patchytonsils, often tender lymphadenopathy,
+++
Complications suppurative (early)
Non-suppurative (late)
2. 12
FACTS Management
•
4
4
4
4
4
4
•
4
•
4
General management :
Rest, oral fluids, and warm saline gargling (for soothing effect).
Analgesics and antipyretics may be used for relief of pain or pyrexia. Acetaminophen
is the drug of choice.
Nasal drops : Normal saline drops may help in young children (<2 yrs) but
Oxymetazoline and Xylometazoline may be sparingly used in older children as short
term nasal congestion relievers.
Anesthetic gargles and lozenges, such as benzocaine, may be used for
symptomatic relief of odynophagia.
Rhinorrhea : The first generation anti-histaminics may relieve rhinorrhea by 25-30%
due to their anti-cholinergic action. Second generation anti-histaminics are poorer.
Cough : Anti-histaminics may help in reducing secretions and preventing post nasal
drips. Cough suppressants (Dexmethorphan, Codeine) and expectorants (Guaifenesin,
Ammonium citrate, Ambroxol, etc.) have not proved to be effective in metanalysis. Use
of cough medication should be predicated by severity of symptoms.
Supportive measures :
Avoidance of irritants (e.g., smoke)
Specific treatment of bacterial infections
Antimicrobial treatment : GABHS Pharyngo-tonsillitis is a self limiting disease
recovering within 3-4 days
The goals of pharmacotherapy are to reduce morbidity and to prevent
complications. 10 days treatment with Penicillin is the therapy of choice.
4
While Penicillin is the drug of choice Amoxycillin is a good alternative
and used widely.
TABLE : WHO Recommended treatment for Acute Gr. A Streptococcal Pharyngitis
(Penicillin-allergic) :
Antibiotic (route) (days)
Erythromycin ethylsuccinate (oral) (10 days)
Azithromycin (oral) (5 days)
First generation Cephalosporin (oral) (10 days)
Children
40-50 mg/kg/day BID /TID
12 mg/kg od
Cefaclor / Cephalexin in usual doses.
1) Short courses of Cefuroxime given in routine doses for 5 days may be as effective as a
ten day course of Penicillin/Amoxycillin
2) C. diphtheriae, N.gonococcus, H. Influenzae, Pneuococcus if isolated should be treated
according to sensitivity reports.
Pharyngo-tonsillitis
1
•
4
4
4
4
4
4
4
Surgical intervention : Guidelines for considering tonsillectomy.
Children with seven or more infections of the tonsills/adenoids in a year despite
adequate medical therapy.
Peritonsillar abscesses
More than four or five episodes of infections per year over a period of two years.
Chronic tonsillitis : Sore throat with tonsillar inflammation for three months duration
Airway obstruction
Chronic EBV infection
Grossly asymmetric tonsils.
13
ACT
How does one manage Pharyngo-tonsillitis?
TABLE : WHO Recommended treatment for Acute Gr. A Streptococcal
Pharyngitis (Non-allergic) :
Antibiotic (route)
Penicillin V (Oral)
Amoxycillin (Oral)
Benzathine penicillin G (IM)
Children (< 30kg) (days)
250 mg BID x 10 days
40 mg/kg/day x 10 days
6 lakh Units (single dose)
Children (> 30kg) (days)
500 mg BID x 10 days
250 mg TID, can be given bid
12 Lakh Units. (single dose)
Examine ears, eyes, nose, throat, body
Red eyes, Rhinitis, Exanthema,
Diarrhea, Hoarseness, Cough +++
Viral (likely)
Purulent , Patchy tonsils,
Tender lymphadenopathy, No cough,
Toxicity +++
1
Bacterial (exclude epiglottitis, diphtheria)
3
Antibiotics & Throat swab
- VE
Symptomatic treatment for 3-4 days
Response No response +VE
RADT
Wait for throat swab before
2
starting antibiotics
Pharyngo-tonsillitis
1
• General management is detailed on the opposite page
1) One should not miss features of diphtheria (e.g. membrane, exceptionally more
toxicity, bull neck, myocarditis etc.)
2) Antibiotics may be withheld for 2 days awaiting culture report. Rheumatic fever
may be prevented even if Penicillin is started upto 9 days of symptoms.
Post-streptococcal glomerulonephritis is a self-limiting disease and use of
antibiotics does not change its occurrence.
Antibiotic therapy
Recommended treatment for those allergic to penicillin is detailed in Table
on page 12 (under ‘FACTS’)