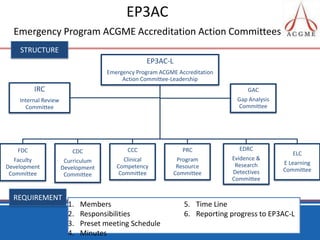
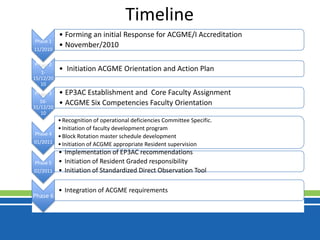
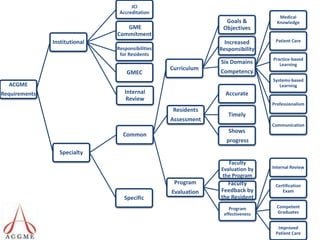
The document outlines an orientation and action plan for an emergency medicine residency program to achieve and maintain accreditation from the Accreditation Council for Graduate Medical Education (ACGME). It discusses forming committees to address the over 70 accreditation requirements in areas such as curriculum, faculty, evaluations, and quality improvement. Timelines and responsibilities are defined for leadership committees to monitor progress and ensure adherence to accreditation standards.


![Residents’ Scholarly Activities The curriculum must advance residents’ knowledge of the basic principles of research, including how research is conducted, evaluated, explained to patients ,and applied to patient care. Residents should participate in scholarly activity. [As further specified by the Advanced Specialty Program Requirements] The sponsoring institution and program should allocate adequate educational resources to facilitate resident involvement in scholarly activities. [As further specified by the Advanced Specialty Program Requirements]](https://image.slidesharecdn.com/acgmeactionplan-101211140254-phpapp01/85/Acgme-action-plan-17-320.jpg)