1. Original Article
Risk factors associated with longer stays in
cardiovascular surgical intensive care unit
after CABG
Kai-Di Kao a,b
, Shiu-Yu Katie C. Lee b,
*, Chieh-Yu Liu c
,
Nai-Kuan Chou d,
**
a
Department of Nursing, National Taiwan University Hospital, Taiwan
b
School of Nursing, National Taipei University of Nursing and Health Sciences, Taiwan
c
Department of Speech Language Pathology and Audiology, National Taipei University of Nursing and
Health Sciences, Taiwan
d
Department of Cardiovascular Surgery, National Taiwan University Hospital, Taiwan
Received 1 September 2020; received in revised form 13 January 2021; accepted 25 April 2021
KEYWORDS
CABG;
Length of stay;
TISS;
Demand of intensive
care;
Quality of care
Background/Purpose: Monitoring ICU length of stay (LOS) after CABG and examining its risk
factors can guide initiatives on the improvement of care. But few have evaluated this issue
to include personal and clinical factors, and demands of ICU care. This study applied Donabe-
dian model to identify risk factors for longer ICU stays after CABG. Lifestyle, clinical factors
during and after CABG, TISS were viewed as structure factors, and infection and organ failures
during ICU did as process factors.
Methods: This retrospective cohort study used data via medical records at a medical center. A
stratified randomized sample of 230 adults from a cohort of 690 isolated CABGs was to reflect
the rate of 34.7% longer than 3-day-ICU LOS. The sample comprised of longer-stay group (n Z
150) and shorter-stay group (n Z 80).
Result: Hierarchical logistic regression analysis revealed that potential signs of infection (3-
day average WBC higher than 10,000/mL, OR: 3.41 and the body temperature higher than 38
C, OR:5.67) and acute renal failure (OR: 8.97) remained as the most significant predicted fac-
tors of stay longer than 3 ICU days. Along with higher TISS score within 24 hours (OR:1.06),
structure factors of female gender (OR:4.16) smoking(OR: 4.87), higher CCI before sur-
gery(OR:1.49), bypass during CABG (OR:3.51) had higher odds of risk to stay longer.
* Corresponding author. 365 Ming-Te Rd., Pei-Tou, Taipei, Taiwan. Fax: þ886 2 2821 3233.
** Corresponding author. Department of Surgery, National Taiwan University Hospital, No. 7 Chung-Shan S. Road, Taipei, Taiwan. Fax: þ886
2 23956934.
E-mail addresses: shiuyu@ntunhs.edu.tw (S.-Y.K.C. Lee), nickchou@ntu.edu.tw (N.-K. Chou).
+ MODEL
Please cite this article as: K.-D. Kao, S.-Y.K.C. Lee, C.-Y. Liu et al., Risk factors associated with longer stays in cardiovascular surgical
intensive care unit after CABG, Journal of the Formosan Medical Association, https://doi.org/10.1016/j.jfma.2021.04.020
https://doi.org/10.1016/j.jfma.2021.04.020
0929-6646/Copyright ª 2021, Formosan Medical Association. Published by Elsevier Taiwan LLC. This is an open access article under the CC
BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.jfma-online.com
Journal of the Formosan Medical Association xxx (xxxx) xxx
2. Conclusion: Further quality improvement initiatives to shorten ICU stay after CABG may
include the promotion of a smoking cessation program in clinical practice, and better manage-
ment of the manpower allocation, infection control and renal failure.
Copyright ª 2021, Formosan Medical Association. Published by Elsevier Taiwan LLC. This is an
open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-
nc-nd/4.0/).
Introduction
The continuous monitoring of critical care indicators and
the identification of risk factors that might lower quality
are essential to improving patient care. The Institute of
Medicine has suggested making efforts to improve the use
of resources,1
and that length of stay should be addressed
to improve critical care quality.2
Longer intensive care unit
(ICU) stay is not only costly and utilization of limited re-
sources, but it also leads to poor patient and family out-
comes. In addition, it hinders self-care abilities, prolongs
rehabilitation time, reduces quality of life, and makes it
more difficult for patients to return to their original roles
and work. Patients may even experience problems caused
by social isolation, that impacts on the function of the
entire family and increases the mortality rate.3e8
Length of
ICU stay is an important indicator of the quality of critical
care for patients who have received a coronary artery
bypass grafting (CABG). Therefore, building a predictive
model for longer cardiovascular ICU stays is necessary for
continuous quality improvement.
Few studies have addressed the factors relating to CABG
patients and treatment, or proposed model-based guides for
improving the quality of care. The Donabedian model has
been widely used. It allows both researchers and policy-
makers to conceptualize the underlying mechanisms and to
identify risk factors that may confirm the true of quality of
care.9
Donabedian proposed a model composing of structure,
process and outcomes for assessing the quality of care. He
assumed that structure indicators have effects on process
that influences the patients’ outcomes. Common structure
indicators may include patients’ characteristics, human
resources and organizational structures that affect the
context in which treatment and care takes place. The
process indicators reflect aspects of how the care is actu-
ally provided.10
Clinicians will need to determine the as-
sociation among indicators in the structure, the process and
the outcome indicators in arriving at any quality improve-
ment initiative.
In previous studies, process outcomes for CABG have
comprised length of stay, quality of life, organ failures and
mortality rate in ICU under the influence of structure and
process factors.3,5,7,8,11,12
The personal factors, such as age,
gender and smoking, the pre-surgery profile, such as Charl-
son comorbidity index (CCI), albumin, hemoglobin, cardiac,
liver and kidney function before surgery, and the charac-
teristics of CABG, such as types of operation, length of time
receiving cardiopulmonary bypass, operative time and blood
transfusion units, as well as the Therapeutic Intervention
Scoring System (TISS) and cardiac output after operation
were proved as risk factors for the ICU stays after
CABG.1,3e8,13e18,29,39,40
They can be regarded as structure
indicators. Nevertheless, the care being received or the
adverse events during ICU that have been proved as risks for
longer length of stay (LOS) can be viewed as process factors
which including organ function such as PaO2/FiO2 ratio,
Creatine kinase-MB (CK-MB), Creatinine, Aspartate amino-
transferase (GOT), and infection sings during the ICU stays.
In addition, indicators that reflecting manpower during
ICU stay, such as nurseepatient ratio and staffing are also
common structure indicators for the quality of ICU
care,20,21
indicating that higher nurse-patient ratio in-
creases the rate of ICU infection or mortality and decreases
the survival rate.16e23
However, few studies have investi-
gated the demand for care or workload in ICU after CABG,
which commonly is measured with the Therapeutic Inter-
vention Scoring System (TISS).18
TISS bases on the principle
that the number of therapeutic interventions is the relation
to the patients’ complexity and severity of a clinical con-
dition, and is an indicator of nursing workload in the
ICU.17,19e21,23
Workload or demand of care is a prerequisite
for the availability and quality of critical care services and
viewed as one of common indicators of strained ICU ca-
pacity.17,19,23
Higher TISS showed the higher rate of adverse
events and higher strained ICU capacity.23,24
In this study,
we used the TISS in the structure factors to explore the
demand for care.
This study based on the Donabedian model9
to identify
risk factors for the longer ICU stays after CABG. The findings
may allow for proactive steps aiming at preventing or
reducing the incidence of modifiable factors in patients
scheduled for CABG for increasing the efficient allocation of
ICU resources.
Methods
This was a retrospective cohort study involving the review
of medical records from the cardiovascular center in a
tertiary medical center, the National Taiwan University
Hospital. To explore the risk factors for long ICU stays,
variables associated with the longer ICU stays after CABG
were determined based on literature reviews and were
grouped according to the Donabedian model (Fig. 1). We
examined all the medical records at the same period to
avoid bias from environmental, policy, and human factors.
This study was approved by the Research Ethics Committee
of the National Taiwan University Hospital.
Sample
A stratified, randomized sample of 230 adults from a cohort
of 690 pure CABGs in the cardiovascular center was
K.-D. Kao, S.-Y.K.C. Lee, C.-Y. Liu et al.
+ MODEL
2
3. included in this study. A longer ICU stay is defined as staying
more than 3 days after CABG, following Ettema et al.12
and
the clinical guidelines of the research institute. Patients
enrolled were 18 years old and had received only CABG
for the first time. Patients were excluded if they had un-
dergone complex cardiac surgery, required extracorporeal
membrane oxygenation support after the operation, re-
operative CABG, readmission, or had incomplete data
such as missing data on each laboratory exams that might
influence the analysis.
A total of 639 patients met the selection criteria, of
which 34.7% (n Z 222) had stayed in the ICU for 3 days
after CABG. To analyze the differences between two
groups, a sample size of 230 was estimated via G Power 3.1
for providing 80% power to obtain 1.5:1 odds of the
outcome, based on Herman’s study.13,28
Stratified ran-
domized sampling strategy was applied to represent the
prevalence of longer ICU stays after CABG in the research
institute and also to minimize the data collection burden.
We randomly selected 150 (65.2%) patients with an ICU stay
of 3 days (n Z 417) and 80 (34.8%) patients with an ICU
stay of 3 days (n Z 222) (Fig. 1).
Instrument
A standardized data collection tool was developed and
based on the review of literature to measure risk factors for
longer ICU stays after CABG. It included patients’ de-
mographics, lifestyle, and disease and treatment data from
the surgery and ICU care. This tool was confirmed for its
content suitability and relevance by a panel of senior
physicians and advanced practice nurses.
Data included, as structure indicators, those affecting
the context of CABG care such as gender, age, BMI, CCI,
nutrition status (albumin, hemoglobin) and information
regarding life style habits, hypertension and hyperlipid-
emia, all of which are consistently associated with
comorbidity of cardiovascular disease.3,6e8,17,23,27e29,39,40
In addition, organ function of the heart, lungs, liver and
kidneys that was evaluated before CABG surgery were
collected.3,6e8,17,23,27e29
The data that indicating as the
structure factors of pre-operation and intra-operation
included the inotropic infusion and IABP inserted before
operation, total operating time, whether cardiopulmonary
bypass being received and the units of blood transfused
during CABG, and TISS scores within 24 hour after ICU
admission.
Data for the process factors included 3-day averaged
laboratory values for organic function, including creatinine
kinase (CK), creatinine kinase MB (CK-MB), ratio of arterial
oxygen partial pressure to inspired oxygen fraction (PaO2/
FiO2 ratio), total bilirubin, creatinine, white blood cell (WBC)
count and body temperature via SwaneGanz catheter. Those
represent risk of infection, organic function and comorbidity
of CABG followed with the US Centers for Disease Control
and Prevention guidelines (Fig. 2).1,5e8,13,14,17,30,31
Data analysis
All data were analyzed using SPSS 22.0 software (SPSS Inc,
Chicago, IL, USA). In univariate analyses, independent-
sample t tests, chi-square tests were used to examine the
differences between the two groups with regard to personal,
lifestyle, intra-operation and ICU factors. Regard to previous
study findings and Donabedian’s model, there is complex
association, interaction among demographics/lifestyle, dis-
ease factors and surgery factors on the ICU process and ICU
stays. Multivariate hierarchical logistic regression was
applied; and the order of factor entry into the model
building is based on Donabedian’s Model. Based on the the-
ory for this study, hierarchical logistic regression allows us to
assess the multivariate effects of ICU care beyond the de-
mographics and disease factors; and to clarify whether the
change in the coefficient when adding other indicators from
Figure 1 Sampling flowchart.
Journal of the Formosan Medical Association xxx (xxxx) xxx
+ MODEL
3
4. personal, pre-operation, intra-operation and post-operation
or ICU process indicators is statistically significant.41,42
Sequentially, we entered the structure factors (Fig. 2)
separately as 2 groups; firstly, personal status and pre-
operation indicators entered for model 1, following with
intra-operation indicator for model 2. Details were shown in
Fig. 2. Due to the TISS score only available at the first 24-
hour ICU measure in the research institute, thus, post-
operation structure of TISS was entered with ICU process
factors at last for model 3. We excluded hemoglobin and
IABP for model 1 because of their multicollinearity with al-
bumin (cramer’s V Z .456 9) and the nature of operation
(cramer’s V Z .749). Rare indicators such as inotropic drugs
and IABP were excluded. Age was not entered independently
since it was weighted in the CCI calculations. Other signifi-
cant factors shown in Table 1 were entered for model
building. A p value of .05 indicated statistical significance
and two-tailed multivariate analyses was used to calculate
adjusted odds ratios (ORs).
Results
Of the 230 participants who received CABG, the average
length of stay was 3.8 2.7 days, ranging from 2 to 42 days.
Of these, 73% were men, and the mean age was 67.5 12.0
years. Regarding chronic diseases, a majority of patients in
each group had the general characteristics of coronary ar-
tery disease, including hypertension and hyperlipidemia
and smoking. The CCI was the mean of 2.8 2.2 (Table 1).
Subjects in the longer-stay group were older (p Z .002),
more commonly female (p Z .009), smoking (p Z .032),
and more likely to have other heart disease (p Z .003), or
hypertension (p Z .011). They also had higher CCI and
lower BMI, lower hemoglobin lower Albumin, and lower
mean LVEF (all p .001). The procedure of CABG in the
longer group was more likely to be emergency, and to use
inotropic drugs and IABP before operation (all p .001).
They also were more likely to had cardiopulmonary bypass
and to had less blood transfusions during CABG (all
p .001). Post-operatively, the longer group had higher
TISS score within 24-hour ICU stay (p .001), lower cardiac
output (p .001), impair PaO2/FiO2 ratio (p Z .005),
higher CK-MB (p .001), higher total bilirubin (p .001),
higher creatinine (p .001), higher body temperature
(p .001), and higher WBC on day 3 (p .001) (Table 1).
Risk factors for ICU stay of ‡3 days after CABG
The 3-step hierarchical logistic regression (Table 2)
revealed, after adjusting for other structure and ICU pro-
cess indicators, that together the personal factors of
gender, smoking and CCI, the intra-operation factor of
bypass during CABG, and the post-operation factors of TISS
score, creatinine and infection signs contributed signifi-
cantly for the longer-than-3-day ICU stay after CABG.
The ICU process indicators, the averaged creatinine level
greater than 2.0 mg/dL was associated with an 8.97-fold risk
of longer ICU stay as compared with the counterpart (DOR,
95%CI, 2.79e28.84, p .001). A 3-day average WBC higher
than 10,000/mL revealed 3.41 times higher risk to stay ICU
longer than 3 days (DOR, 95%CI, 1.40e8.32, p .001) and
did the body temperature higher than 38
C a 5.67-time
higher risk (DOR, 95%CI, 1.12e28.33, p .001).
Among personal structure factors, gender, CCI and
smoking remained to have effect on longer ICU stays after
CABG. Being female was significantly more likely to stay
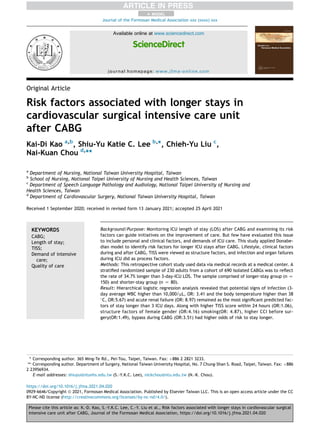
Figure 2 Framework of predicting risk factors for longer ICU stay after CABG based on the Donabedian’s model. Abbreviation:
ICU Z intensive care unit; CCIZ Charlson Comorbidity Index; GOT Z aspartate aminotransferase, LVEF Z left ventricular ejective
rejection; CABG Z coronary artery bypass graft, IABPZ Intra-aortic balloon pumping; TISS Z Therapeutic Intervention Scoring
System, CK-MB Z creatine kinase-MB; 3rd WBCZ White Blood Cell count on day 3 after CABG surgery.
K.-D. Kao, S.-Y.K.C. Lee, C.-Y. Liu et al.
+ MODEL
4
5. Table 1 Group comparison of structure and process factors based on Donabedian’s model (N Z 230).
Total ICU length of stay
3 days (n Z 150) 3 days (n Z 80) p-value
Structure- Personal and pre-operation
Age, MSD 67.5 12 65.7 11.4 70.9 12.2 .002
Gender, n (%) .009
Male 178 (77.4%) 124 (82.7%) 54 (67.5%)
Female 52 (22.6%) 26 (17.3%) 26 (32.5%)
Smoking, n (%) .032
Yes 168 (73%) 102 (60.7%) 66 (78.5%)
No 62 (27%) 44 (39.3%) 18 (21.5%)
CCI a
2.8 2.2 2.3 2.1 3.6 2.2 .001
BMI(m2
) 24.8 3 25.4 3.2 23.6 3.9 .001
Albumin 4.3 .5 4.4 .4 4.1 .5 .001
Hemoglobin 12.9 2 13.0 2.0 12.5 2.0 .047
GOT 46.4 95.5 39.8 103.1 54.6 75.8 .43
Total Bilirubin .86 .55 .86 .55 .88 .55 .79
Creatinine 1.7 1.7 1.6 1.5 1.7 1.7 .67
LVEF 52.1 15.5 54.8 13.2 46.4 15.1 .001
Combine other heart disease, n (%) .003
Yes 21 (9.1%) 7 (4.7%) 14 (17.5%)
No 209 (90.9%) 143 (95.3%) 66 (82.5%)
Hypertension, n (%) .011
Yes 162 (70.4%) 114 (76%) 48 (60%)
No 68 (29.6%) 36 (24%) 32 (40%)
Hyperlipidemia, n (%) .254
Yes 89 (38.7%) 63 (42%) 26 (32.5%)
No 141 (61.3%) 87 (58%) 54 (67.5%)
Stent insertion, n (%) .53
Yes 177 (77%) 112 (74%) 65 (81%)
No 53 (23%) 38 (26%) 15 (19%)
Inotropic infusion, n (%) .001
Yes 9 (3.9%) 1 (0.7%) 8 (10%)
No 221 (96.1%) 149 (99.3%) 72 (90%)
IABP inserted, n (%) .001
Yes 18 (7.8) d
5 (3.3%) 13 (16.3%)
No 212 (92.2%) 125 (96.7%) 67 (83.8%)
Nature of operation .001
Scheduled, n (%) 203 (88.3%) 143 (95.3%) 60 (75%)
Emergency, n (%) 27 (11.7%) 7 (4.7%) 20 (25%)
Intra-operation
Length of operation (hour) 7.6 2.3 7.5 2.1 7.7 2.7 .615
Bypass during CABG, n (%) .001
Yes 66 (28.7%) 27 (18%) 39 (48.8%)
No 164 (71.3%) 123 (82%) 41 (51.2%)
Blood transfusion, n (%) .001
Yes 173 (75.2%) 101 (67.3%) 72 (90%)
No 57 (24.8%) 49 (32.7%) 8 (10%)f
TISS score within 24-hour 41.4 19.5 38.6 7.66 43.6 9.3 .001
Process e ICU (Post-operation)
Cardiac output a
4.6 1.5 4.8 1.02 4.1 1.0 .001
Hemoglobin a
11.6 1.3 11.7 1.35 11.6 1.3 .17
PaO2/FiO2 ratio a
268 (122.9) 276.1 120.1 252.9 127.6 .005
CK-MB a
31.8 64.9 19.9 43.7 44.7 60.8 .001
Total bilirubin ac
1.4 0.9 1.2 0.7 1.6 1.3 .001
Creatinine a
2.1 1.3 1.4 1.2 2.0 1.4 .001
Temperature b
37.5 .7 37.3 .4 37.6 .4 .001
(continued on next page)
Journal of the Formosan Medical Association xxx (xxxx) xxx
+ MODEL
5
6. longer at SICU than being male (DOR, 95%CI, 1.22e14.18,
p Z .023). Higher CCI score had 1.49 times higher odds of
risk for stay ICU longer than 3 days (DOR, 95%CI, 1.21e1.85,
p .001). Current smokers had 4.87 times higher risk than
non-smoker did. The adjusted odds even increased
sequentially if adjusted for intra-operation indicators in
Model 2 and further adjusted for ICU structure and process
indicators in Model 3 (Table 2).
Among intra- and post-operation structure indicators,
received cardiopulmonary bypass during CABG and TISS
score within 24-hour ICU were significant risk factors.
During the operation, bypass during CABG extended ICU
stay 3.5 times (DOR, 95%CI, 1.29e9.54, p .001). A high
TISS score within 24 hours extended ICU stay 1.06 times
(DOR, 95%CI, 1.00e1.12, p .001).
Discussion
The risk factors for long ICU stay after CABG are complex
and multifold; few studies have focused on a model-based
analysis identifying such factors. This study provides evi-
dence identifying risk factors for extended ICU stays to
support continuous improvement of quality of care in the
ICU. The main findings of this study were as followed, after
adjusting for personal and operation factors, being female,
smoking, higher CCI, receiving bypass during CABG, higher
TISS score, impaired kidney function, and potential infec-
tion signs were proven as risk factors predicting an
increased length of stay in the ICU. Supported with the CCI
weighted for age, we have demonstrated that age, along
with other chronic illness, viewed as CCI contributes
Table 1 (continued)
Total ICU length of stay
3 days (n Z 150) 3 days (n Z 80) p-value
3rd WBCG (k/ul) c
11.6 3.6 10.85 32.2 12.5 43.8 .001
Data presented as mean SD for continuous variables and percentage for categorical variables.
Note: a
average of 3 days on each variable; b
Temperature: 3-day average checked via SwaneGanz catheter after CABG surgery; c
3rd
WBCG: white blood cell count on day 3 after CABG surgery d
Fisher’s exact test.
Abbreviation: CCI Z Charlson Comorbidity Index; GOT Z Aspartate aminotransferase; LVEF Z left ventricular ejective rejection;
CABG Z coronary artery bypass graft; IABPZ Intra-aortic balloon pumping; TISS Z Therapeutic Intervention Scoring System; PaO2/FiO2
ratio; CK-MB Z Creatine kinase-MB.
Table 2 Multivariate hierarchical logistic regression of risk factors for longer ICU stay after CABG (N Z 230).
Statistics methods variables Multivariate logistic regression
Model 1 Model 2 Model 3
Adjusted OR (95% CI) Adjusted OR (95% CI) Adjusted OR (95% CI)
Structure
Personal pre-operation
Gender: Female vs Male 4.24 (1.62e11.12) ** 4.09 (1.48e11.27) * 4.16 (1.22e14.18) *
Smoking Yes vs no 3.19 (1.19e8.55) * 3.55 (1.27e9.94) * 4.87 (1.39e17.05) *
CCI 1.30 (1.11e1.52) * 1.33 (1.12e1.57) * 1.49 (1.21e1.85) ***
Hypertension yes v.s. no 0.50 (.25e1.01) 0.45 (.21-.97) * Not significant
Emergency operation yes v.s. no 5.57(1.89e16.44) ** 4.68(1.47e14.87) ** Not significant
Intra-operation
Bypass during CABG yes v.s. no 3.17 (1.46e6.867) ** 3.51 (1.29e9.54) *
TISS score within 24 hour 1.06 (1.00e1.12) *
Process e ICU (Post-operation)
Creatinine group (Cr)
Cr:1.2 reference
Cr:1.3w1.9 2.19 (.86e5.62)
Cr 2.0 8.97 (2.79e28.84) ***
3rd WBCG e
3.41 (1.40e8.32) **
Temperature 5.67 (1.12e28.33) *
Note:*p .05; **p .01; ***p .001.
Model 1: adjusted for BMI, Albumin, Combined other heart disease, and LVEF.
Model 2: adjusted for model 1 and blood transfusion.
Model 3: adjusted for model 2 and Cardiac outputs, CK-MB, PaO2/FiO2 ratio, total bilirubin.
Abbreviation: CCI Z Charlson Comorbidity Index, CABG Z coronary artery bypass graft, TISS Z Therapeutic Intervention Scoring
System.
K.-D. Kao, S.-Y.K.C. Lee, C.-Y. Liu et al.
+ MODEL
6
7. significantly on longer stay in CVSICU. Even controlling for
smoking, intra-operative and ICU process factors, older with
major chronic illness increased odds to stay longer in ICU.
Studies often identify factors similar to those identified
in our study, particularly structural indicators pointing to
promotion of preventive programs for cardiovascular disease
or screening for operation risk. Older age, being male and
having chronic illnesses such as hypertension, diabetes,
respiratory failure and prolonged mechanical ventilation,
impaired renal function, recurring myocardial infarction,
and poor cardiac (e.g., LVEF 30%) have all been demon-
strated to be predictors of longer ICU stays after isolated
CABG.3,29e31
Nevertheless, the fact of being female
revealed a different trend in our study. We found that only
one-third of the study sample was female, but they pre-
sented much higher risks of needing to stay longer in ICU
than men (female v. s. male DOR: 4.16, 95% CI:1.22e14.18).
We further explored the gender differences in this research
sample (Table 3) and found that women had higher CCI (3.63
v. s. 2.53; p Z .043) and inotropic infusion (9.6% v. s. 2.2%;
p Z .001) before operation, more blood transfusion during
operation (88% v. s. 71%, p Z .011), and lower cardiac
output (3.87 v. s. 4.74, p .001) and higher creatinine level
(88% v. s. 71%, p Z .011) after operation. This gender dif-
ference has consistently shown itself in the gender differ-
ence for ICU mortality after CABG. Recent Ettema’s
systematic review,38
similar to Beckers’ long-term anal-
ysis,31
reveals that despite the trend of lower mortality from
CABG, the remaining women had higher mortality than
men.34
Females in our study may have faced a higher chal-
lenge in ICU recovery as they presented higher TISS scores,
generally worse post-operative cardiac and renal function
than men did after other disease factors being controlled. In
addition, it also echoes the delays in the use of medical care
by domestic women.
Our study shown smoking is a risk factor for longer ICU
stays after cardiac surgery, as supported in other stud-
ies.14,15,25e33,38
Moreover, the threat of smoking on longer
Table 3 The gender difference on demographic, pre-, intra-, and post-operation (N Z 230).
Female (n Z 52) Male (n Z 178) p-value
Mean SD/n (%) Mean SD/n (%)
Demography and pre-operation
Age 70.1 (10.22) 66.7 (12.3) .078
Smoking Yes 17 (33) 151 (62) .001
Combine other heart disease Yes 16 (31) 73 (41) .016
Hypertension Yes 39 (75) 123 (69) .491
Hyperlipidemia Yes 16 (30.8) 73 (41) .199
CCI 3.63 (1.63) 2.53 (2.28) .001
BMI(m2
) 23.9 (3.41) 25.03 (3.58) .053
Albumin 4.21 (.54) 4.36 (.47) .055
Hemoglobin 13.3 (1.82) 12.73 (2.06) .001
Total bilirubin .74 (.5) .90 (.56) .67
Creatinine 1.43 (1.41) 1.67 (1.62) .73
LVEF 50.21 (13.38) 52.37 (14.7) .345
Emergency operation Yes 6 (11.5)f
21 (11.8) .98
Inotropic infusion Yes 5 (9.6) d
3 (2.2) .03
IABP Yes 2 (3.8) 16 (9) .387
CAD with LAD Yes 51 (98.1) 170 (95.5) .462
Intra-operation
Bypass during CABG Yes 19 (37) 47 (26) .166
Blood transfusion Yes 46 (88) 127 (71) .011
TISS score within 24 hour 41.29 (8.3) 40.06 (8.68) .364
Post-operation
Cardiac output a
3.87 (.94) 4.74 (1.01) .001
Hemoglobin a
10.98 (1.28) 11.82 (4.01)
PaO2/FiO2 ratio a
324.95 (84.58) 287.03 (84.33) .005
CK-MB a
27.17 (28.8) 28.97 (56.59) .826
Creatinine a
1.96 (1.55) 1.46 (1.05) .008
Total bilirubin a
1.23 (.91) 1.34 (.94) .434
Temperature b
37.40 (.43) 37.4 (.36) .885
3rd WBC (k/ul) c
11.2 (39.52) 11.4 (37.01) .727
Data presented as mean SD for continuous variables and percentage for categorical variables.
Note: a
average of 3 days on each variable; b
Temperature: 3-day average checked via SwaneGanz catheter after CABG surgery; c
3rd
WBC: white blood cell count on day 3 after CABG surgery; d
Fisher’s exact test.
Abbreviation: CCI Z Charlson Comorbidity Index; LVEF Z left ventricular ejective rejection; IABPZ Intra-aortic balloon pumping; CADZ
Coronary artery disease; LAD Z Left anterior descending; CABGZCoronary artery bypass graft, TISS Z Therapeutic Intervention Scoring
System, CK-MB Z creatine kinase-MB.
Journal of the Formosan Medical Association xxx (xxxx) xxx
+ MODEL
7
8. ICU stays is moderated by risks in operation and ICU pro-
cess, as the adjusted OR was 4.87 in the final model from
model 1 (DOR: 3.19) in hierarchical regression. Smoking has
been associated with increased delirium, lung complica-
tions, wound infection, multisystem failure and mortality
rates.38
Zhang and colleagues also found that smoking was
an independent predictor of the composite endpoint of
death, MI or stroke after PCI or CABG, with hazard ratio of
1.8 (95% CI: 1.3 to 2.5).34
Thus smoking may be a moder-
ating factor of longer ICU stay and should receive more
attention; and smoking cessation should be proactively
promoted during ICU stays.
Hypertension is significant in univariate analysis, but
trajectory result in multivariate analysis from model 1 to
model 3 is no significance. It may be the adjust effect of the
variables (other organ functions and infection related fac-
tors after surgery) which was put into model 3. It also
showed that appropriate care on controlling blood pressure
before operation may decreased the incidence of longer
ICU stay after CABG.
In spite of the improvement in surgical technique, the
process of CABG, particularly the bypass, remains a risk for
longer ICU stay after controlling the structure indicators or
ICU care in this study.28,35
In previous studies, fibrillation,
pulmonary dysfunction, renal complications, and adverse
received longer anesthesia, operation time, cardiopulmo-
nary bypass time, and intubation time (p .05 for all
comparisons) emerged as the factors for longer ICU stay.28
It
may be because CPB may induce many negative effects such
as systematic inflammatory response syndrome, atrial cere-
bral effects, and the rate of revascularization etc. and lower
survival rate.30,37
Thus, it is suggested to pay more attention
to monitoring organ function after CPB in ICU care.
In the post-operation phase of care, the result indicated
that higher TISS score, impaired kidney function, potential
infection signs such as WBC higher than 10,000/mL and body
temperature higher than 38
C on day 3 were predictors of
longer ICU stays after CABG. TISS score represents a complex
condition in the critical care unit composed of several items in
both active treatment and non-active treatment, such as
bleeding and blood infusion, hemodialysis, vasoactive drug
infusion, multiple dressing changes, routine drug infusion,
chest physiotherapy, etc.16e18,21,23,36
TISS score indicates the
demands of ICU care that is related to the complexity and
severity of illness, particularly related to utilization of care or
workload.18,21,23
Higher TISS score is a risk for longer ICU stay
and mortality rate, and is one indicator of strained ICU ca-
pacity affecting the ICU’s ability to provide high quality care,
but the proportion of understaffing did not differ between
survivors and non-survivors.21,23,40
Poor renal function may
lead to hemodialysis that may increase the demand of care in
unstable patients after operation, as it may manifest acidosis,
impaired urine output or higher creatinine level. Similarly to
Almashrafi’s systematic review study3
and Eltheni’s study,27
our study reveals higher creatinine level, a manifestation of
renal failure, is a predictor of longer ICU stays. Thus, appro-
priate manpower allocation for those higher TISS score and
higher creatinine levels are suggested to meet the high de-
mands of ICU care after CABG and to reduce the incidence of
prolonged ICU stays.
Moreover, potential signs of infection are strong predictors
of longer ICU stay in this study. Several studies reported pa-
tients with signs of potential infection will not only prolong
their ICU stay, but they also induced a higher mortality
rate.19,20,32
Lagercrantz et al.1
studied Swedish patients over
a 5-year period who were discharged after a stay in ICU
longer than 10 days. Their survival rate was only 52% and the
most common causes of death were infection, stroke and
multiple organ failure. Friedrich et al.32
also reported that
patients who stayed in the ICU for over 7 days had increased
infection rates in BSI (31.5%), VAP (28.1%), UTI (22.5%), and
surgical wound infection (10.6%). Thus, infection control is
still an important quality indicator in ICU care, and clinicians
need to review the bundle care of infection regularly.
The multi-step of hierarchical logistic regression in our
study found that smoking, poor infection control and renal
failure were the three greatest risk factors for longer ICU
stay after CABG, that also increase the demand of
manpower allocation. We suggested that smoking cessation
is necessary before surgery because it was the most factor
associated with longer ICU stay in this study. Also,
manpower allocation for those patients with higher TISS
scores in critical care units should be carefully reconsid-
ered, and signs of potential infection should be addressed
before and after cardiac surgery.
Some limitations remain to be considered. Although the
study used a theory-guided approach to identify risk factors
and applied stratified random sampling to represent the
prevalence rate of longer-than-3-day ICU stay in this
research institute, the findings may present a particular
center as the data gathered form a single, tertiary CVS ICU
in Taipei, Taiwan. Patients in this center might have been
suffering from more similar or sever conditions during the
study period. Clinical application should be cautious. In
addition, the limitation of secondary data and the chart
review process should be stressed. The assessment of
lifestyles and history of major chronic illness may not
have standardized in the clinical setting, though the
availability and accuracy of the standard procedure for
data abstraction was verified.
Further studies are also warranted as this issue is multi-
factorial. If more research resource is available, case-
matched, nested strategies to control some factors for
model building and the validation of the predicting model in
another sample can contribute better for the true of quality
and the continuous quality improvement of the CABG care.
Declaration of competing interest
No conflict of interest with non-financial interest.
References
1. Lagercrantz E, Lindblom D, Sartipy U. Survival and quality of
life in cardiac surgery patients with prolonged intensive care.
Ann Thorac Surg 2010;89(2):490e5.
2. Institute of Medicine Committee on Quality of Health Care in A.
Crossing the quality chasm: a new health System for the 21st
century. Washington (DC): National Academies Press (US)
K.-D. Kao, S.-Y.K.C. Lee, C.-Y. Liu et al.
+ MODEL
8
9. Copyright 2001 by the National Academy of Sciences; 2001. All
rights reserved.
3. Almashrafi A, Elmontsri M, Aylin P. Systematic review of factors
influencing length of stay in ICU after adult cardiac surgery.
BMC Health Serv Res 2016;16:318.
4. Kapadohos T, Angelopoulos E, Vasileiadis I, Nanas S,
Kotanidou A, Karabinis A, et al. Determinants of prolonged
intensive care unit stay in patients after cardiac surgery: a
prospective observational study. J Thorac Dis 2017;9(1):70e9.
5. Azarfarin R, Ashouri N, Totonchi Z, Bakhshandeh H, Yaghoubi A.
Factors influencing prolonged icu stay after open heart sur-
gery. Res Cardiovasc Med 2014;3(4). 2-2.
6. Oliveira EK, Turquetto AL, Tauil PL, Junqueira Jr LF, Porto LG.
Risk factors of prolonged hospital stay after isolated coronary
artery bypass grafting. Braz J Cardiovasc Surg 2013;28(3):
353e63.
7. Mahesh B, Choong CK, Goldsmith K, Gerrard C, Nashef SA,
Vuylsteke A. Prolonged stay in intensive care unit is a powerful
predictor of adverse outcomes after cardiac operations. Ann
Thorac Surg 2012;94(1):109e16. 6.
8. Almashrafi A, Alsabti H, Mukaddirov M, Balan B, Aylin P. Factors
associated with prolonged length of stay following cardiac
surgery in a major referral hospital in Oman: a retrospective
observational study. BMJ Open 2016;6(6):e010764.
9. Donabedian A. The qualirt of care. How can be it assessed? J
Am Med Assoc 1988;260:1743e8.
10. Donabedian A. Evaluating the quality of medical care. 1966.
Milbank Q 2005;83(4):691e729.
11. Cacciatore F, Belluomo Anello C, Ferrara N, Mazzella F,
Manzi M, De Angelis U, et al. Determinants of prolonged
intensive care unit stay after cardiac surgery in the elderly.
Aging Clin Exp Res 2012;24(6):627e34.
12. Ettema RG, Peelen LM, Schuurmans MJ, Nierich AP,
Kalkman CJ, Moons KG. Prediction models for prolonged
intensive care unit stay after cardiac surgery: systematic re-
view and validation study. Circulation 2010;122(7):682e9. 687
pp. following p. 689.
13. Herman C, Karolak W, Yip AM, Buth KJ, Hassan A, Légaré JF.
Predicting prolonged intensive care unit length of stay in pa-
tients undergoing coronary artery bypass surgery–development
of an entirely preoperative scorecard. Interact Cardiovasc
Thorac Surg 2009;9(4):654e8.
14. Sharif-Kashani B, Shahabi P, Mandegar MH, Saliminejad L,
Bikdeli B, Behzadnia N, et al. Smoking and wound complica-
tions after coronary artery bypass grafting. J Surg Res 2016;
200(2):743e8.
15. Bayfield NGR, Pannekoek A, Tian DH. Preoperative cigarette
smoking and short-term morbidity and mortality after cardiac
surgery: a meta-analysis. Heart Asia 2018;10(2):e011069.
16. Keene AR, Cullen DJ. Therapeutic intervention scoring System:
update 1983. 1983. 0090-3493 (Print)).
17. Padilha KG, Sousa RM, Kimura M, Miyadahira AM, da Cruz DA,
Vattimo Mde F, et al. Nursing workload in intensive care units:
a study using the Therapeutic Intervention Scoring System-28
(TISS-28). Intensive Crit Care Nurs 2007;23(3):162e9.
18. Liang YW, Tsay SF, Chen WY. Effects of nurse staffing ratios on
patient mortality in Taiwan acute care hospitals: a longitudinal
study. J Nurs Res 2012;20(1):1e7.
19. Dancer SJ, Coyne M, Speekenbrink A, Samavedam S,
Kennedy J, Wallace PG. MRSA acquisition in an intensive care
unit. Am J Infect Contr 2006;34(1):10e7.
20. Blatnik J, Lesnicar G. Propagation of methicillin-resistant
Staphylococcus aureus due to the overloading of medical
nurses in intensive care units. J Hosp Infect 2006;63(2):162e6.
21. Lee A, Cheung YSL, Joynt GM, Leung CCH, Wong WT,
Gomersall CD. Are high nurse workload/staffing ratios associ-
ated with decreased survival in critically ill patients? A cohort
study. Ann Intensive Care 2017;7(1):46.
22. Rewa OG, Stelfox HT, Ingolfsson A, Zygun DA, Featherstone R,
Opgenorth D, et al. Indicators of intensive care unit capacity
strain: a systematic review. Crit Care 2018;22(1):86.
23. Jansson M, Ohtonen P, Syrjala H, Ala-Kokko T. The proportion
of understaffing and increased nursing workload are associated
with multiple organ failure: a cross-sectional study. J Adv Nurs
2020;76(8):2113e24.
24. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power
analyses using G*Power 3.1: tests for correlation and regression
analyses. Behav Res Methods 2009;41(4):1149e60.
25. Ji Q, Zhao H, Mei YQ, Shi YQ, Ma RH, Ding WJ. Impact of
smoking on early clinical outcomes in patients undergoing
coronary artery bypass grafting surgery. J Cardiothorac Surg
2015;10(16).
26. D’Hoore W, Bouckaert A, Tilquin C. Practical considerations on
the use of the Charlson comorbidity index with administrative
data bases. J Clin Epidemiol 1996;49(12):1429e33.
27. Eltheni R, Giakoumidakis K, Brokalaki H, Galanis P, Nenekidis I,
Fildissis G. Predictors of prolonged stay in the intensive care
unit following cardiac surgery. ISRN Nurs 2012;2012:691561.
28. Passaroni AC, Silva MA, Yoshida WB. Cardiopulmonary bypass:
development of John Gibbon’s heart-lung machine. Rev Bras
Cir Cardiovasc : Orgao Off Soc Bras Cir Cardiovasc 2015;30(2):
235e45.
29. Tunç M, S
‚ahuto
glu C, Karaca N, Kocabas
‚ S, As
‚kar FZ. Risk factors
for prolonged intensive care unit stay after open heart surgery
in adults. Turkish J Anaesthesiol Reanim 2018;46(4):283e91.
30. Benedetto U, Kamel MK, Khan FM, Angelini GD, Caputo M,
Girardi LN, et al. Are racial differences in hospital mortality
after coronary artery bypass graft surgery real? A risk-adjusted
meta-analysis. J Thorac Cardiovasc Surg 2019;157(6):2216e25.
e2214.
31. Becker ER, Granzotti AM. Trends in in-hospital coronary artery
bypass surgery mortality by gender and race/ethnicity –1998-
2015: why do the differences remain? J Natl Med Assoc 2019;
111(5):527e39.
32. Friedrich JO, Wilson G, Chant C. Long-term outcomes and
clinical predictors of hospital mortality in very long stay
intensive care unit patients: a cohort study. Crit Care 2006;
10(2):R59.
33. Saxena A, Shan L, Reid C, Dinh DT, Smith JA, Shardey GC, et al.
Impact of smoking status on early and late outcomes after
isolated coronary artery bypass graft surgery. J Cardiol 2013;
61(5):336e41.
34. Zhang YJ, Iqbal J, van Klaveren D, Campos CM, Holmes DR,
Kappetein AP, et al. Smoking is associated with adverse clinical
outcomes in patients undergoing revascularization with PCI or
CABG: the SYNTAX trial at 5-year follow-up. J Am Coll Cardiol
2015;65(11):1107e15.
35. Okano R, Liou Y-J, Yu H-Y, Wu IH, Chou NK, Chen YS, et al.
Coronary artery bypass in young patients-on or off-pump? J
Clin Med 2019;8(2):128.
36. Muehler N, Oishi J, Specht M, Rissner F, Reinhart K, Sakr Y.
Serial measurement of Therapeutic Intervention Scoring
System-28 (TISS-28) in a surgical intensive care unit. J Crit
Care 2010;25(4):620e7.
37. Benedetto U, Albanese A, Kattach H, Ruggiero D, De Robertis F,
Amrani M, et al. Smoking cessation before coronary artery
bypass grafting improves operative outcomes. J Thorac Car-
diovasc Surg 2014;148(2):468e74.
38. Bukkapatnam RN, Yeo KK, Li Z, Amsterdam EA. Operative
mortality in women and men undergoing coronary artery
bypass grafting (from the California Coronary Artery Bypass
Grafting Outcomes Reporting Program). Am J Cardiol 2010;
105(3):339e42.
39. Stoppe C, Goetzenich A, Whitman G, Ohkuma R, Brown T,
Hatzakorzian R, et al. Role of nutrition support in adult cardiac
surgery: a consensus statement from an international
Journal of the Formosan Medical Association xxx (xxxx) xxx
+ MODEL
9
10. multidisciplinary expert group on nutrition in cardiac surgery.
Crit Care 2017;21(1):131.
40. Chermesh I, Hajos J, Mashiach T, Bozhko M, Shani L, Nir RR,
et al. Malnutrition in cardiac surgery: food for thought. Eur J
Prev Cardiol 2014;21(4):475e83.
41. Henderson HV, Velleman PF. Building multiple regression
models interactively. Biometrics 1981;37(2):391e411.
42. Kerlinger FN. Foundations of behavioral research. New York:
Holt, Rinehart and Winston; 1986.
K.-D. Kao, S.-Y.K.C. Lee, C.-Y. Liu et al.
+ MODEL
10