1. Methodology and Results
Drivers of readmission
in post solid organ transplant population
Background of Problem
Purpose
The purpose of this study is to describe a process that a transplant department, involved in
the coordination of care for transplant patients undertook to identify drivers of readmission
in post solid organ transplant population (heart , lung and liver transplants specifically).
SRTR reports that > 40% of post-transplant patients are readmitted within the first year of
their transplant. However, this number is underreported because admission data reported
is limited to admission in the transplant center and excludes admission events occurring
outside of the transplant center. This creates silos that lead to fragmentation of care and
inadequate reporting of actual readmission events. Prospective review of more complete
patient data facilitates predicting patients at risk for readmission and guides the
development of timely intervention and addressing patient needs early on to prevent
readmissions.
Ultimately, the goal is to develop a future state in data analytics that moves transplant data
analysis from descriptive and diagnostic analytics to predictive analytics that will transform
how care is provided post transplant.
Factors explaining LOS of either the transplant surgery admission or the post-transplant
readmission in order of significance (p-value between .00001 and .04) were 1)ESRD/
dialysis 2)MCS as bridge to transplant 3)Hepatorenal syndrome, and 4)Bed-to-bed transfer
to the transplant center.
Phase III
Based on these results, further study was done on a cohort of patients transplanted from
2009-2012 to focus on explaining LOS of the post-transplant readmissions. Transplant
surgery LOS (p<.001) and dialysis (p=.001) were both significant in a regression
where the dependent variable was total number of readmission days within 1 yr
post-transplant.
Understanding the patterns and risk factors for readmissions post solid organ
transplantation is an essential step toward creating internal strategies and overarching
regional policies in the overall management post transplant. Although not all readmissions
post transplant are avoidable, ensuring that patient needs are met in various care settings
will ensure appropriate utilization of healthcare services. Further studies are needed to
explore the reasons for higher readmission rates in some groups of patients with specific
diagnoses. Additionally, more studies are needed to test the use of predictive analytics to
help providers anticipate the needs of patients as well as accurately predict the level of
care needs. The ultimate goal is to provide timely and appropriate care for patients who
received solid organ transplantation that prolongs the life of the graft, minimizes the long
term effects and sequelae of post transplant immunosuppression and improves quality of
life.
References
Ladner, D. P., Skaro, A. I. and Abecassis, M. M. (2012), Are all readmissions the same? Liver Transpl 2012;18:1007–1008
Pereira AA, Bhattacharya R, Carithers R, Reyes J, Perkins J. Clinical factors predicting readmission after orthotopic liver transplantation. Liver Transpl 2012;18:1037-1045
National Transplant Services
Transplantation is known to be costly but a necessary and effective treatment of end stage
conditions. Hospitalization readmission after discharge post-transplant is sometimes
unnecessary and avoidable. Having the ability to identify factors that contribute to
readmissions and increase in length of stay will help define specific interventions in
post-transplant care.
Conclusion and Recommendation
Phase I
A retrospective review of post transplant hospitalizations on patients transplanted from
2009-2011 demonstrated a positive correlation between readmission up to1 year post-
transplant and a longer length of stay (LOS) of the transplant surgery.
Phase II
Subsequently, prospective data collection was done from March through December
2013 to identify specific drivers of readmissions post transplant.
Clinical and demographic data collected were:
General: discharge location (home, SNF, ARU), bed to bed transfer, re-transplant w/in 30
days, status of transplant event (de-novo, redo), intubation prior to transplant surgery,
hospitalization w/in 90 days prior to transplant, highest education, denied by other
transplant center, dialysis
Liver: MELD at admission, MELD at transplant, hepatorenal syndrome, hepato-pulmonary
syndrome
Heart: Mechanical circulatory device
Lung: LAS at transplant
Malou Valencia, MSN, CNS, National Transplant Services, Director, California Transplant Hubs-NCAL SCAL NW & HI regions
Larcy Caguin, MSN, FNP, National Transplant Services, High-risk transplant coordinator
Marmi Le, MBA, National Transplant Services, Healthcare Data Analyst
Elaine Perez, RN, BSN, CCTC; Kenni Bishop, RN, BSN; Eboni Clark, RN, MSN, National Transplant Services, Operation Managers for SCAL, NCAL, and CEAST Hubs
To find patterns and risk factors that predispose patients for readmission 90 days
from day of discharge post-transplant, a retrospective chart review was done on a
subset of 119 charts drawn from the previous cohorts. A more focused approach was
undertaken to review cases where LOS from the transplant surgery to discharge was 30
days or greater. Clinical variables were added to the data collection including co-
morbidities such as DM 2, history of neurologic conditions, GI complications and other GI
related issues, acute kidney injury (AKI), CRRT, surgical complications, infections
(including SBP), thrombosis, alcohol cirrhosis, social support, depression, HCC, hepatic
encephalopathy, graft dysfunction, and pulmonary issues.
Next, t-tests were performed to see if the average number of readmission days for
patients having a certain factor was significantly different than for those without the factor.
Factors were tested on their own and as interaction variables (e.g. patient was a bed to
bed transfer AND had encephalopathy). Although HCV and alcohol related cirrhosis were
not statistically significant when tested explicitly, they may have contributed to a LOS of
the transplant event >30 days, which was a significant variable.
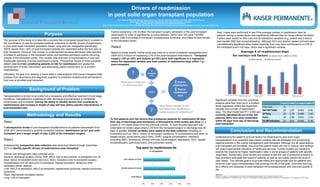
Significant variables from the univariate
analysis were then tried out in a multiple
linear regression where the dependent
variable was number of readmission
days. The final model had R2 = 0.544 and
correctly identified 88 out of the 102
patients (86%) who were readmitted
within 90 days from day of discharge
post-transplant.
Coef t Stat P-value 95% CI
Intercept 0
AKI*HD*ESRD 22 1.97 0.052 0-45
GI*Surg 24 2.79 0.006 7-42
Pulm 19 2.58 0.011 5-34
TE>30*Infection 22 2.61 0.010 5-39