1. 1
OH
N O
N
N
S
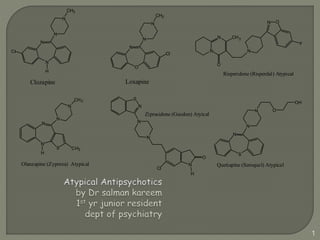
Clozapine Loxapine
CH3
N
N
H
S CH3
N
N
Cl
CH3
N
N
N
O
Cl
CH3
H
N
N
N
N
Olanzapine (Zyprexa) Atypical
O
F
CH3
N O
N
N
N
H
Cl
O
N
N
N
S
N
Risperidone (Risperdal) Atypical
Quetiapine (Seroquel) Atypical
Ziprasidone (Geodon) Atyical
2. Other names
• 2nd generation
• Serotonin Dopamine Antagonists
Features
• Higher ratio of serotonin : dopamine receptor
blockade
• Appear more specific for mesolimbic than striatal
dopamine system
3. Developments in Medical Treatments
for Psychotic Disorders
’30s ’40s ’50s ’60s ’70s ’80s ’90s ’00 ’02
ECT
Haloperidol
Fluphenazine
Thioridazine
Chlorpromazine
Loxapine
Perphenazine
Clozapine
Risperidone
Olanzapine
Quetiapine
Ziprasidone
Aripiprazole
Next-generation
First-generation
antipsychotics Second-generation
antipsychotics
ECT = electroconvulsive therapy.
Kapur and Remington. Ann Rev Med. 2001;52:503.
Worrel et al. Am J Health Syst Pharm. 2000;57:238.
5. Atypical Antipsychotics In Vivo Binding Affinities
Low D2 receptor blocking effects
Reduced risk of extrapyramidal side
Healoffpeercidtsol. Clozapine Risperidone Olanzapine
Quetiapine Ziprasidone
5HT2A D2 D1 Alpha 1 Musc H1 5HT1A (agonist)
Casey 1994
6. Schizophrenia and schizoaffective disorder
– acute and chronic psychoses
• Treatment of severe tardive dyskinesia (clozapine)
Mood disorder – acute mania
• OLANZAPINE – bipolar disorder
• Augments anti depressants in acute management
of depression.
7. Other indications
• Exhibits outwardly aggressive and violent behaviour
• Autistic spectrum disorder
• Tourettes syndrome
• Huntington’s disease
• Lesch Nyhan Syndrome
• Along with methylphenidate/dextroamphetamine in
children with ADHD.
• Psychosis secondary to head trauma, dementia,
treatment resistant
• Decreases the risk of suicide and water intoxication in
patients with schizophrenia
10. Sexual dysfunction
• result from NE and SE blockade
• erectile dysfunction in 23-54% of men
• retrograde ejaculation
• loss of libido and anorgasmia in men and women
Seizures - <1% for generalized grand mal
11. Adverse pharmacologic effects of antipsychotic drugs.
Type Manifestations Mechanism
Autonomic
nervous
system
Loss of accommodation, dry
mouth, difficulty urinating,
constipation
Muscarinic cholinoceptor blockade
Orthostatic hypotension,
impotence, failure to ejaculate
Alpha adrenoceptor blockade
Central
nervous
system
Parkinson's syndrome, akathisia,
dystonias
Dopamine receptor blockade
Tardive dyskinesia
Supersensitivity of dopamine
receptors
Toxic-confusional state Muscarinic blockade
Endocrine
system
Amenorrhea-galactorrhea,
infertility, impotence
Dopamine receptor blockade
resulting in hyperprolactinemia
Other Weight gain
Possibly combined H1 and 5-HT2
blockade
12.
13. Benzisoxazole
Undergoes first pass metabolism
Peak plasma level levels – 1 hr (parent
compound) , 3 hrs for
metabolite
Combined half life 20 hrs (once daily
dosing)
Antagonist of serotonin 5HT2A, dopamine
D2, α1, α2 adrenergic histamine H1
receptors.
15. Dosages – Initially 1-2 mg/day , raised to 4 mg/
day
Only SDA available in depot formation IM injection
every 2 weeks (25mg,50mg or 75 mg)
Drug interactions – Paroxetine and Fluoxetine
(blocks the formation of
RISPERIDONE’S active
metabolite)
RISPERIDONE + SSRI – significant elevation of
prolactin - galactorrohea and breast enlargement
16.
17. 85% absorbed from the GI tract
40% is inactivated by first pass metabolism
Peak concentration - 5hrs
Half life - 31 hrs
5HT2A ,D1, D4, α1 ,5HT1A , muscarinic M1
through M5 and H1 receptors
19. Periodic assessment of “blood sugar” and
“transaminase”.
Increased stroke among patients with
dementia
DOSAGES – initial dose for treatment of
psychosis – 5-10 mg , acute mania- 10-15
mg.
• Start 5-10 mg , raise to 10 mg per day
• 30-40 mg in treatment resistant cases.
20. Drug interactions
• FLUVOXAMINE and CIMETIDINE – increases
• CARBAMAZEPINE and PHENYTOIN - decreases
21. DIBENZOTHIAZEPINE
Rapidly absorbed from GI tracts
Peak plasma concentration – 1-2 hrs
Steady half life – 7 hrs (2- 3 dosing per
day)
lower-potency compound with relatively
similar antagonism of 5-HT2, D2, α1, and α2
receptors .
22. Side effects
• – somnolence, postural hypotension and
dizziness – most common side effect.
• Least likely to cause extra pyramidal side effects.
– used in Parkinsonism who develop DOPAMINE
AGONIST induced psychosis.
• Moderate weight gain
• Small rise in heart rate , constipation and transient
rise in liver transaminases can occur.
23. DOSAGES – available in 25, 50 and 200
mg.
Schizophrenia – target of 400 mg/ day
Mania & BPD – 800 & 300 mg respectively
Insomnia – 25- 300 mg at night
24. BENZOTHIAZOLYL PIPERAZINE
Peak plasma concentration- 2-6 hrs
Terminal half life at steady state – 5-10 hrs
Bioavailability doubles when taken along
with food.
Blocks 5HT2A and D2 receptors , antagonist
5HT1D, 5HT2C, D3,D4,α1 and H1 receptors.
25. Agonist activity at 5HT1A receptor
Serotonin reuptake inhibotor
Nor epinephrine reuptake inhibitor
Side effects –
• somnolence, headache, dizziness , nausea , light
headedness, prolongation of QTc interval.
• avoided in patients with cardiac arrythmias.
26. Dosages – 20,40, 60 ,80 mg.
IM comes single use daily 20mg/ml vial
Oral ziprasidone initiated at 40 mg a day.
Efficacy in the range of 80-160 mg/day.
High as much as 240 mg are being used.
27.
28. DIBENZODIAZEPINE
Rapidly absorbed
Plasma level – 2 hrs
Steady state – less than one week if twice
daily dosing is used.
Half life – 12 hrs
Antagonist of 5HT2A , D1,D3,D4 and α
receptors.
33. • AGRANULOCYTOSIS
Leucocyte and differential blood count normal before
starting
Monitor counts every week for 6 months, then at
least Q 2 weeks after 1 year
At least Q 4 weeks after count stable for 1 year (for 4
more weeks after discontinuation)
If leucocyte count < 3000/mm3, or if ANC <
1500/mm3, discontinue immediately and refer to
hematologist
Patient should report immediately symptoms of
infection, esp. flu-like illness (fever, sore throat)
34. Dosages
• Initial dosage is 25 mg one or 2 times daily
although conservative initial dosage is 12,5 mg
daily.
• Raised gradually to 25 mg a day for every 2-3
days to 300 mg divided doses
• 900 mg can be used.
• Plasma conc greater than 350 ng/mL is likely hood
for better response.
35. Drug interactions
• Clozapine + (carbamazepine, phenytoin,
propulthiouracil, sulfonamides, captopril) causes
bone marrow suppression.
• Clozapine+ Lithium – increases the risk of
seizures, confusion and movement disorders.
• Clozapine+ Paroxetine – precipitate clozapine
associated neutropenia.
37. Therapeutic indications
• Schizophrenia - maintenance treatment for 15-30
mg
• Acute mania –
• Other uses – add on for SSRI in treatment of
mood disorder cases.
• Oppositional defiant disorder or conduct disorder.
38. CYP3A4
inducer
Increase in clearance and lower blood levels dose
must be increased (doubled).
e.g. carbamazepine
CYP3A4
inhibitor
Decrease in clearance and higher blood levels. dose
must be decreased (one-half).
e.g. ketoconazole
CYP2D6
inhibitor
Decrease in clearance and higher blood levels. dose
must be decreased (one-half).
e.g. quinidine, fluoxetine, paroxetine
39. Bifeprunox - partial dopamine agonist.
• Treatment of schizophrenia
• GI side effects are most common.
Paliperidone – major active metabolite of
resperidone.
• Recommended dose of 6mg per day with 3-12
mg/day.