
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Final production conn's
Similar to Final production conn's (20)
Recently uploaded
Recently uploaded (20)
Final production conn's
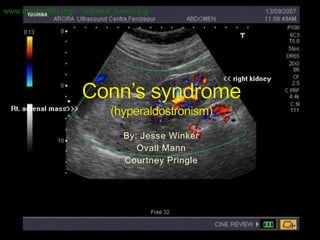
- 1. www.mcghealth.org/.../adrenal_tumor.jpg By: Jesse Winker Ovall Mann Courtney Pringle
- 2. Conn’s syndrome is an Adosterone- Producing Adenoma. Conn’s syndrome named after American endocrinologist Jerome W. Conn. Condition was first described at the University of Michigan in 1955
- 5. Conn’s Syndrome is a disease that effects the adrenal glands. It involves excess production of a hormone called aldosterone. (which is the hormone that regulates sodium and potassium reabsorption by the cells of the tubular portion of the kidney.)
- 6. Essential hypertension can mimic Conn's syndrome. Conn’s syndrome can also be lead to the buffalo hump (Cushing syndrome) Therefore high blood pressure and low blood potassium may be due to essential hypertension, which is being treated with diuretic drugs that cause a loss of potassium in the urine.
- 7. Conn’s syndrome normally effect most people in their 30- 60 years of age. Conn’s syndrome is normally found in female cases then male. Conn syndrome occurs in 50- 60% of cases of primary hyperaldosteronism. image1.masterfile.com/.../82/700- 00528234w.jpg
- 8. Frequent urination (polyuria) Increased thirst Weakness and fatigue Headache Muscle cramps Tingling in fingers Temporary paralysis Heart palpitations Hypertension (high blood pressure) adrenalstressblog.wordpress.com/
- 9. You can identify it on a MRI The appearance of the tumor on CAT scans www.med- ed.virginia.edu/.../anatomy/adrenal.html diagnosticimaging.com
- 10. www.surgicaloncology.com/a tf034c.jpg The goal of treatment is to lower blood pressure.(any other symptom) If tumor appears on gland then the gland will be removed.(laparoscopic surgery) All symptoms associated with Conn’s syndrome are resolved and further treatment involves controlling blood pressure . www.mcghealth.org/.../adrenal_tumor.jpg
- 11. Most adrenal disease requiring surgery can be done using minimally invasive (laparoscopy) surgery techniques. Laparoscopic adrenalectomy is the preferred technique for non-cancerous adrenal disease, including the following: Aldosterone-secreting adrenal tumors (Conn's syndrome) Cortisol-secreting adrenal tumors (Cushing's syndrome) Adrenalin-producing adrenal tumors (Pheochromocytoma) Primary adrenal hyperplasia Adrenal hyperplasia after failed treatment of Cushing's disease Large nonfunctioning adrenal tumors (<10-12cm) Adrenal metastasis
- 12. www.rfay.com.au/images/laparoscopy.jpg performed under a complete general anesthesia. A cannula (a narrow tube-like instrument) is placed into the abdominal cavity in the upper abdomen or flank just below the ribs. A laparoscope (a tiny telescope) connected to a special camera is inserted through the cannula. This gives the surgeon a magnified view of the patient's internal organs on a television screen. Other cannulas are inserted which allow your surgeon to delicately separate the adrenal gland from its attachments. Once the adrenal gland has been dissected free, it is placed in a small bag and is then removed through one of the incisions. It is almost always necessary to remove the entire adrenal gland in order to safely remove the tumor. After the surgeon removes the adrenal gland, the small incisions are closed.
- 13. After surgery patient usually cared for by a surgical nursing unit. Usually enlisted into intensive care to monitor he patient blood woldfitness.com pressure. Patients with an aldosterone- producing tumor will need to have their serum potassium level checked after surgery Patients cortisol-producing tumors need to take prednisone or cortisol http://normalpotassiumlevels.com/meas uring-blood-potassium-levels
- 14. http://www.sages.org/publication/id/PI14/ http://surgery.wustl.edu/Surgery_M.aspx?id=976&me nu_id=178 http://www.instablogsimages.com/1/2011/09/02/pills_ and_pills_kwia3.jpg http://emedicine.medscape.com/article/117280- overview www.mcghealth.org/.../adrenal_tumor.jpg
Editor's Notes
- Patients