Presentation1.pptx, radiological imaging of peri natal acute ischemia and hypoxic ischemic leukoencephalopathy.
•Download as PPTX, PDF•
31 likes•2,723 views


Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Presentation1.pptx, radiological imaging of peri natal acute ischemia and hypoxic ischemic leukoencephalopathy.
Similar to Presentation1.pptx, radiological imaging of peri natal acute ischemia and hypoxic ischemic leukoencephalopathy. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Presentation1.pptx, radiological imaging of peri natal acute ischemia and hypoxic ischemic leukoencephalopathy.
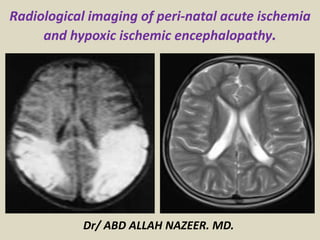
- 1. Radiological imaging of peri-natal acute ischemia and hypoxic ischemic encephalopathy. Dr/ ABD ALLAH NAZEER. MD.
- 2. Perinatal acute Stroke, similar to a stroke which occurs in adults, is defined as a disturbance to the blood supply of the developing brain. This description includes both ischemic events, which results from a blockage of vessels, and hypoxic events, which results from a lack of oxygen to the brain tissue, as well as some combination of the two. A neonatal stroke occurs in approximately 1 in 4000 births, but is likely much higher due to the lack of noticeable symptoms. One treatment with some proven benefits is hypothermia, but may be most beneficial in conjunction with pharmacological agents. Neonatal strokes may lead to cerebral palsy, learning difficulties, or other disabilities. Well-designed clinical trials for stroke treatment in neonates are lacking, but some current studies involve the transplantation of neural stem cells and umbilical cord stem cells; it is not yet known if this therapy is likely to be successful.
- 3. Risk Factors: Many different risk factors play a role in causing a neonatal stroke. Some maternal disorders that may contribute to neonatal strokes include: autoimmune disorders, coagulation disorders, prenatal cocaine exposure, infection, congenital heart disease, diabetes, and trauma. Placental disorders that increase the risk of stroke include placental thrombosis, placental abruption, placental infection, and chorioamnionitis. Other disorders that may increase the risk of a neonatal stroke are blood, homocysteine and lipid disorders, such as polycythemia, disseminated intravascular coagulopathy, prothrombin mutation, lipoprotein (a) deficiency, Factor VIII deficiency, and Factor V Leiden mutation. Infectious disorders such as central nervous system (CNS) infection or systemic infection may also contribute. Many infants who suffer a neonatal stroke also follow an uncomplicated pregnancy and delivery without identifiable risk factors, which exemplifies the necessity for further research on this subject.
- 4. Perinatal arterial ischemic stroke (PAIS) has an estimated incidence of 1 in 2,300 live births. Most often PAIS presents with convulsions. Initial assessment is performed with (Doppler) ultrasound and amplitude-integrated electroencephalography (aEEG). Magnetic resonance imaging (MRI) is used to confirm PAIS. Although neonatal MRI enables prediction of motor outcome in PAIS patients by localizing the stroke area according to the posterior limb of the internal capsule or by visualizing pre-Wallerian degeneration, it remains difficult to determine the viability of brain tissue after stroke. In adults it has been shown that arterial spin labeling (ASL) perfusion MRI, a noninvasive technique, is valuable for the assessment of acute stroke. Perfusion deficits and perfusion– diffusion mismatches as visualized on the ASL images have been proven to correspond with dynamic susceptibility contrast-enhanced images. Furthermore, a relation between perfusion in the affected hemisphere and outcome has been shown. Although noninvasive ASL perfusion imaging seems to be a promising tool in the neonatal population, experience is still limited, and only one study has described the use of ASL MRI in the evaluation of PAIS. ASL MRI could demonstrate areas of hypo- and hyperperfusion in patients with PAIS. However, ASL has not yet been used to assess changes in perfusion (abnormalities) over time in neonates with stroke. In addition, regional cerebral oxygenation (rScO2) was monitored, compared with reported rScO2 values in neonates (63 ± 12% , and analyzed as a function of the perfusion signal as visualized on the ASL MR images.
- 5. Radiographic features CT diffuse edema with effacement of the CSF-containing spaces decreased cortical gray matter attenuation with loss of normal gray-white differentiation decreased bilateral basal ganglia attenuation reversal sign: reversal of the normal CT attenuation of grey and white matter, demonstrated within the first 24 hours in a small number of these patients it has been proposed that this finding is due to the distention of deep medullary veins secondary to partial obstruction of venous outflow from the elevated intracranial pressure caused by diffuse edema the end result is that the cerebral white matter is of higher attenuation than the cortical gray matter white cerebellum sign: has been described in at least one study as a component of the reversal sign and in which there is diffuse edema and hypoattenuation of the cerebral hemispheres with sparing of the cerebellum and brainstem, resulting in apparent high attenuation of the cerebellum and brainstem relative to the cerebral hemispheres linear hyperdensity outlining the cortex as well as linear cortical enhancement (later and less evident signs), correspond to cortical laminar necrosis.
- 6. MRI Diffusion-weighted MR imaging is the earliest imaging modality to become positive, usually within the first few hours after a hypoxic- ischemic event due to early cytotoxic edema. During the first 24 hours, there may be restricted diffusion in the cerebellar hemispheres, basal ganglia, or cerebral cortex (in particular, the perirolandic and occipital cortices). The thalami, brainstem or hippocampi may also be involved. Diffusion-weighted imaging abnormalities usually pseudo-normalize by the end of the 1st week . As in younger patients, conventional T1 and T2 weighted images are often normal or demonstrate only very subtle abnormalities. In the early subacute period (24 hours–2 weeks), conventional T2 weighted images typically become positive and demonstrate increased signal intensity and swelling of the injured gray matter structures. T1 hyperintensities signaling cortical laminar necrosis become evident after two weeks. This hyperintense signal does not represent hemorrhage, it's believed to be caused by the accumulation of denatured proteins in dying cells. This hyperintensity can be seen also within a few days on FLAIR.
- 7. Acute Ischemic Stroke. NECT and Axial DWI-diffusion.
- 8. CT of a 7 day old with history of perinatal asphyxia, shows diffuse low attenuating supratentorial brain parenchyma with relatively hyperdense Cerebellum - "CT Reversal sign" of Global hypoxia.
- 9. CT scan show bilateral hypodensity involving the basal ganglia and the thalami Axial T1WI show hyperintensity of the basal ganglia. Axial T2WI shows corresponding hypointensity . DWI reveals hyperintensity at the basal ganglia, hippocampi and occipital lobes, consistent with restricted diffusion of acute ischemic injury.
- 10. CT without and with iv contrast. Axial T2 with bilateral thalamic infarct.
- 11. Global hypoxic-ischemic brain injury.
- 17. Images show the temporal evolution of a right-sided main branch MCA territory infarction (patient 1) on T1-weighted images (top row) and T2-weighted images (bottom row) obtained on days 2, 5, 12, 42, and 75 post-delivery.
- 18. Graph shows DWIs of a patient with an infarction within the PCA territory, showing severe HSI on day 3 (A) and mild-to-moderate HSI on day 10 (B).
- 19. MRI Diffusion show bilateral fronto parietal and parieto occipital cortical restricted diffusion. Similar restricted diffusion in caudate nuclei. Area of involvement corresponds to cortical as well as internal border zone infarcts. Imaging wise : Bilateral border infarcts
- 20. A, Axial T2-weighted fast spin-echo image (3200/85/1), with an echo train length of 8, obtained at 13 hours of life shows no abnormality. B, Trace LSDI image (1520/62.5/1), with a b max of 750 seconds/mm2, obtained at 13 hours of life shows no abnormality. C, Corresponding ADC map. D, Axial T2-weighted fast spin-echo image obtained at 5 days of life shows very subtle hyperintensity in the posterior putamen bilaterally (arrows). E, Trace LSDI image obtained at 5 days of life shows decreased diffusion in corresponding areas (arrows). F, Corresponding ADC map. G, T1-weighted axial spin-echo image (600/20/2) obtained at 6 weeks of life shows hyperintensity within the posterior putamen and ventrolateral thalamus bilaterally (arrows).
- 21. The neonatal mean diffusion-weighted image (mDWI) shows an ischemic area in the middle cerebral artery territory, which resulted in a cyst observed at 3 and 24 mo. The neonatal Z map shows normal Z values in all regions. At 3 mo, low Z values, representing abnormal fractional anisotropy (FA) values, were observed in the affected corticospinal tract, which corresponded with the subsequent development of unilateral motor deficits. The Z map at 24 mo was essentially identical. Interestingly, FA values in the fornix continued to decrease from the time of the neonatal scan to 24 mo, suggesting delayed degeneration in this tract.
- 23. Restricted diffusion signal in the DCST. Left middle cerebral artery infarction (A) results in DWI signal changes throughout the DCST. PLIC and cerebral peduncle involvement are evident on coronal (B) and sagittal images (C). Signal in the basis pontis and medullary pyramids can be seen on left (D) but not right (E) parasagittal sections.
- 24. Neonate with left middle cerebral artery stroke and chronic hemiparesis, DWI signal is appreciated throughout the DCST including PLIC (A), peduncle (B, C), pons (D, E), and pontomedullary junction (F).
- 27. Axial diffusion weighted images from a neonate (A) with a modified pediatric ASPECTS of eight (involvement of left internal capsule, insula, M3, M5, M6, P1, P2, and thalamus) and a child (B) with a modified pediatric ASPECTS of 10 (involvement of left caudate, lentiform, internal capsule, insula, and middle cerebral artery territories M1– M6).
- 28. (A) Axial diffusion-weighted image showing hyperintensity in the territory of left middle cerebral artery. (B) MR angiography demonstrates loss of flow distal to the left middle cerebral artery bifurcation. A B
- 30. Perinatal asphyxia, more appropriately known as hypoxic- ischemic encephalopathy (HIE), is characterized by clinical and laboratory evidence of acute or subacute brain injury due to asphyxia. The primary causes of this condition are systemic hypoxemia and/or reduced cerebral blood flow (CBF). Birth asphyxia causes 840,000 or 23% of all neonatal deaths worldwide HIE- Acute brain injury that occur before, during or after birth. Signs and symptoms: Mild hypoxic-ischemic encephalopathy •Muscle tone may be slightly increased and deep tendon reflexes may be brisk during the first few days •Transient behavioral abnormalities, such as poor feeding, irritability, or excessive crying or sleepiness (typically in an alternating pattern), may be observed •Typically resolves in 24h.
- 31. Moderately severe hypoxic-ischemic encephalopathy The infant is lethargic, with significant hypotonia and diminished deep tendon reflexes. The grasping, Moro, and sucking reflexes may be sluggish or absent The infant may experience occasional periods of apnea Seizures typically occur early within the first 24 hours after birth Full recovery within 1-2 weeks is possible and is associated with a better long-term outcome. Severe hypoxic-ischemic encephalopathy Seizures can be delayed and severe and may be initially resistant to conventional treatments. The seizures are usually generalized, and their frequency may increase during the 24-48 hours after onset, correlating with the phase of reperfusion injury. As the injury progresses, seizures subside and the electroencephalogram becomes isoelectric or shows a burst suppression pattern. At that time, wakefulness may deteriorate further, and the fontanelle may bulge, suggesting increasing cerebral edema.
- 32. Other symptoms include the following: Stupor or coma is typical; the infant may not respond to any physical stimulus except the most noxious. Breathing may be irregular, and the infant often requires ventilatory support Generalized hypotonia and depressed deep tendon reflexes are common Neonatal reflexes (eg, sucking, swallowing, grasping, Moro) are absent Disturbances of ocular motion, such as a skewed deviation of the eyes, nystagmus, bobbing, and loss of "doll's eye" (ie, conjugate) movements may be revealed by cranial nerve examination Pupils may be dilated, fixed, or poorly reactive to light Irregularities of heart rate and blood pressure are common during the period of reperfusion injury, as is death from cardiorespiratory failure An initial period of well-being or mild hypoxic-ischemic encephalopathy may be followed by sudden deterioration, suggesting ongoing brain cell dysfunction, injury, and death; during this period, seizure intensity may increase.
- 35. Imaging of neonatal hypoxic- ischemic encephalopathy. Ultrasonography is the first-line imaging technique for the evaluation of the newborn brain, These past few years have seen an increasing role of MRI in the investigation of HIE because of greater sensitivity and specificity. Electro-encephalogram(EEG). Computed Tomography(CT). MRI, MRS and DWI.
- 36. MRI sequences: T1 WI, T2 WI++ FLAIR: are not very useful to detect lesion in young infant less than 24 months due to brain maturation. IR T1-weighted: Has been very helpful in the last two decades before generalization of high fields MRI as it gives excellent images of brain anatomy and maturation, It also shows accurately the differentiation between myelinated and unmyelinated WM. Three-dimensional GE T1 weighted sequence (3DT1): •allow 1 mm contiguous slices, which can be reconstructed in any anatomic plane. T2: to detect hemorrhagic lesions DWI: It is now recommended that DWI should be performed between 2 days and 8 days of life. Multiple studies have shown : DWI are more sensitive in the detection of HIE lesions than conventional MRI especially for early diagnosis.
- 37. MRI Protocol: Sagittal and axial T1 WI Axial and coronal T2 WI Axial T2* 3D T1 FLAIR (older child) DWI MRS: Lactate peak: •due to anaerobic glycolysis •found within 24 h of life Subsequently, a reduction in N-acetyl aspartate (NAA) is evident due to neuronal loss.
- 38. Advanced technique: Perfusion. Arterial Spin-Labeled (ASL) Perfusion •Recent advances in novel research imaging modality. •allows noninvasive evaluation of CBF (cerebral blood flow) using electromagnetically labeled arterial blood water as an endogenous contrast agent. •Demonstrates low CBF in neonates who have suffered HIE and in infants and children after stroke.
- 39. Imaging Recommendation: Cranial sonography (US): •First, between 7 and 14 days, •Repeat before discharge from the hospital MRI, DWI, MRS •When US is abnormal: MRI precise lesion extension and aide in prognosticating, • Defining injury in VLBW neonates with "normal" US. Prognosis: Poor outcome if : •IVH plus PVL, •PVL with volume loss, widespread infarction, or seizures •PVL with enlarged cysts.
- 42. It is necessary to : •know the normal cerebral appearance before interpret pathological aspect •distinguish hypoxic-ischemic brain damage from normal myelination Brain composition: Changes in brain composition: Changes in cellular density, increase in complex lipids content due to the evolving process of myelination, decrease in water content mostly in the WM Shortening of T1 Shortening of T2
- 53. Imaging Pattern: The imaging patterns of HIE can be classified into 3 types: Lesions predominantly located in the PVWM, Lesions predominantly located in the basal ganglia or thalamus, Multicystic encephalomalcia. The pattern of injury is postulated to depend on : • The type of hypoxia–ischaemia (acute and profound or prolonged and partial). •The gestational age (term or pre-term).
- 54. HIE in preterm infant. Risk Factors: Pregnancy: Gestational age/weight, previous preterm birth, spontaneous preterm labor Intrapartum: Abruption, pre-eclampsia, premature rupture of membranes, chorioamnionitis, group B Strep Peri & postnatal factors: Respiratory distress, sepsis, anemia, apnea, bradycardia, cardiac arrest.
- 55. General Features: ++ PVL +/- associated to: Germinal matrix and IVH PV hemorrhagic infarction Cerebellar infarction Definition: •PVL is the HIE driven periventricular white matter (PVWM) necrosis seen in very low birth weight premies (<1500g). Epidemiology •Birth weight < 1500 g 45% incidence of PVL (higher if associated with IVH) •Gestational age < 33 weeks 38% incidence of PVL •> 50% of patients with PVL or grade III IVH develop cerebral palsy.
- 60. Cranial ultrasound, coronal view, day 1, showing severe echogenicity in the white matter. MRI (T2SE (TR 6284/TE 120) and ADC) performed on day 3 showing increased signal intensity in the white matter on T2SE and low signal intensity in the deep white matter on the ADC map with sparing of the anterior periventricular white matter and asymmetrical distribution in the parieto-occipital white matter. The child died and was subsequently diagnosed to have molybdenum cofactor deficiency.
- 61. Cranial sonography in 5-day old term with HIE with increase in echogenicity of white matter consistent with edema. CD ultrasound shows reversal of diastolic flow, reflecting increased vascular resistance secondary to edema.
- 62. PVL in a preterm infant. (a) Coronal head US image obtained in the 1st week of life shows increased echogenicity in the periventricular white matter (arrows). (b) Follow-up US image obtained 2 months later shows development of cystic changes in these regions and dilatation of the adjacent lateral ventricles, findings that are consistent with PVL.
- 63. CT images show decrease In basal ganglia density related to Cytotoxic edema. Subtle loss of the normally sharp Transition from grey matter to White matter at the corticomedullary Junction . Cerebral edema seen with effacement of the cortical sulci and the sylvian Fissures.
- 67. PVL in a preterm neonate. Axial T1- weighted (a) and T2- weighted (b) MR images obtained on day 4 of life demonstrate T1 hypointensity and T2 hyperintensity in the periventricular white matter. Note the punctate foci of high signal intensity on the T1- weighted image (arrows in a). These foci should be distinguished from foci of hemorrhage, which would demonstrate greater T2 shortening on the corresponding T2- weighted image.
- 68. 28-week-old, 1100-g infant. Initial MR images, A (T2-weighted SE [3000/120/1]) and B–D (T1- weighted SE [400/15/2]), at 38 weeks corrected age show multiple spots of periventricular T1 and T2 shortening (black arrows) with cyst formation (white arrows) and an irregular contour to the ventricular wall. Follow-up MR images, E and F (T2-weighted SE [3000/100/1]), at 15 months postconceptional age reveal marked irregularity of the ventricular wall, white matter loss, and periventricular T2 prolongation (arrows). The infant developed a spastic diplegia.
- 69. 28-week-old 1355-g infant. Initial MR images, A and B (T2-weighted SE [3000/120/1]) and C and D (T1-weighted SE [400/15/2]), at 38 weeks corrected age show large germinal matrix region hemosiderin deposit (arrowhead) with adjacent multiple encephaloclastic cysts (arrows), diffuse hemosiderin deposition along the lateral ventricle, ventriculomegaly, and absence of periventricular parenchymal signal change. Follow-up MR images, E and F (T2-weighted SE [3000/100/1]), at 12 months corrected age reveal right periventricular hemosiderin deposition (arrowheads), ventriculomegaly, and parenchymal destruction involving the left deep gray matter. Also note the periventricular T2 prolongation (arrows) with white matter volume loss. The infant developed a spastic diplegia with hemiparesis.
- 76. HIE in term infant.
- 89. Severe HII in a 6-yearold child. (a) Unenhanced CT scan obtained at the level of the basal ganglia after cardiopulmonary arrest that lasted 30 minutes is essentially unremarkable. (b) On an unenhanced CT scan obtained just inferior to but contemporaneously with a, the cerebellum appears slightly hyperattenuating relative to the rest of the brain. This finding is another example of the white cerebellum sign as an early CT indicator of HII. (c, d) Diffusion- weighted (c) and T2-weighted (d) MR images obtained 4 days later show high signal intensity with corresponding T2 abnormalities in the caudate nuclei (white arrows), lentiform nuclei (black arrows), and occipital lobes (* in c).
- 90. CT Scan show Hyperdense thalami. Cortical atrophy. Ex vacuo dilatation of lateral ventricle with undulating walls suggestive of Gliosis and paucity of periventricular white matter - Periventricular leukomalacia.
- 91. Full-term infant with acute sentinel event (ruptured uterus) with MRI pattern suggestive of acute near total asphyxia. a Inversion recovery sequence (TR 5038/TE 30/TI 600) does not show a normal signal within the posterior limb of the internal capsule, but areas of increased signal intensity within thalami and basal ganglia. DWI (b– d) shows restricted diffusion in the ventrolateral thalami, lentiform nuclei, cerebral peduncles, and in the perirolandic cortex. Also note involvement of the hippocampi.
- 92. Full-term infant with ‘white brain’ pattern of injury. a, c T2SE (TR 6284/TE 120) shows increased signal intensity in the white matter with loss of cortical ribbon. There is relative sparing of the basal ganglia and immediate periventricular white matter. DWI (b, d) confirms the abnormalities and shows a striking discrepancy in signal intensity with the cerebellum. Note high- signal intensity of the mesencephalon (c) on T2SE and symmetrical restricted diffusion in the cerebral peduncles and also in the cerebellum (d).
- 93. A 14yo with delayed milestones showing bilateral peri rolandic cortical and occipital cortical Gliosis suggestive of Perinatal Hypoxic Ischemic injury
- 94. End-stage PVL in a 9-yearold child who presented with motor and cognitive delay and seizures. The patient was born at 32 weeks gestational age. Axial fluid-attenuated inversion recovery MR images demonstrate increased signal intensity and a few tiny cysts in the immediate periventricular white matter. In b, there is enlargement of the atria of the lateral ventricles with a decrease in volume of the adjacent white matter, and the walls of the lateral ventricles have a wavy appearance.
- 95. Color coded white matter directions and FA images. The inset indicates the level of horizontal sections displayed in A and B. Genu most anterior region of the corpus callosum, ALIC anterior limb of the internal capsule, PLIC posterior limb of the internal capsule, Splenium the most posterior portion of the corpus callosum, Isthmus region of the corpus callosum just anterior of the splenium. (A) The colors indicate the direction of white matter fibers with blue left-right, red anteroposterior and green cranial-caudal (point out from the plane of the page). (B) The intensity corresponds to FA. Black corresponds to FA 0 and the higher the FA value the whiter the image.
- 96. Hypoxic-ischemic encephalopathy. From left to right: Bilateral basal ganglia hyperintense rounded signal in axial FLAIR T2 images, with restricted diffusion hyperintense in DW images and with low ADC values.
- 97. Delayed leukoencephalopathy after acute carbon monoxide intoxication.
- 98. Fibre tractography of hypoxic-ischemic leuckoenecephalopathy.
- 99. Sagittal image of a child with PVL grade 1. Transverse and sagittal image of a child with PVL grade 2.
- 100. Sagittal image demonstrating extensive PVL grade 3 Coronal and transverse images demonstrating PVL grade 4.
- 107. Born at 37 weeks, following antenatal diagnosis of fetal supraventricular tachycardia. MRI, T2SE (TR 6284/TE 120) performed on day 3, shows a large left-sided middle cerebral artery infarct of antenatal onset, with evidence of Wallerian degeneration and presence of cysts within the area of infarction. Diffusion tensor tractography shows loss of fibers with the corticospinal tract of the affected hemisphere
- 111. MR spectroscopy. Biochemical analysis of the (compromised anaerobic) cerebral tissues. Elevated lactate and diminished N-acetyl- aspartate NAA concentration. Elevation of choline relative to creatine. Lactate-choline ratio of 1 indicate a greater than 95% probability of adverse neurodevelopmental outcome.
- 112. MR spectroscopy of a single voxel at 35 msec, demonstrate non-specific accumulation of metabolite at 1.2-1.3 ppm. Spectrum at an echo time of 144 msec shows inversion of the same metabolite, which is characteristic for lactate.
- 120. Thank You.