Download as PDF, PPTX
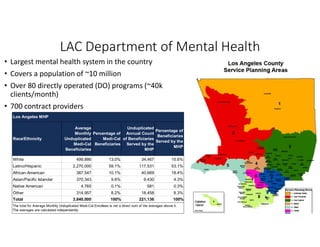

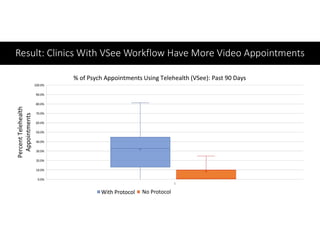

The document discusses the implementation and evolution of telehealth services within the Los Angeles County Department of Mental Health, highlighting demographic statistics of Medi-Cal beneficiaries and the rapid transition to remote care during COVID-19. It outlines the expansion of telepsychiatry services to improve access and redistribute psychiatric resources, with a focus on addressing challenges such as technology access and privacy concerns. Future directions involve enhancing telehealth integration with electronic medical records and addressing unmet needs through customer feedback.























































































