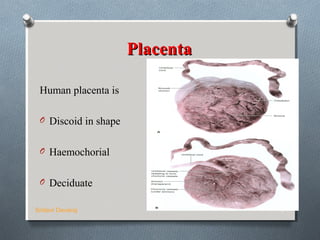
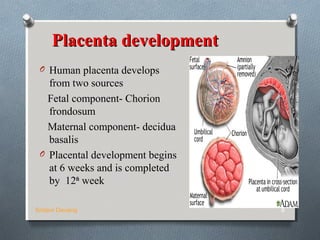
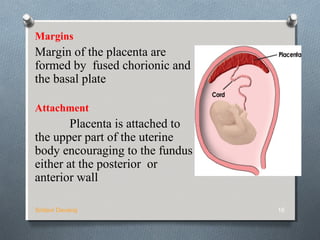
The placenta develops in the uterus during pregnancy and provides oxygen and nutrients to the growing fetus while removing waste products. It attaches to the uterine wall and the umbilical cord arises from the placenta. The placenta develops from the chorionic villi on the fetal side and the decidua basalis on the maternal side. It grows rapidly and eventually replaces most of the decidua basalis. At term, the placenta is a circular disc that is the site of maternal-fetal transfer of oxygen, carbon dioxide, nutrients, waste and various proteins and hormones essential to the development and survival of the fetus.