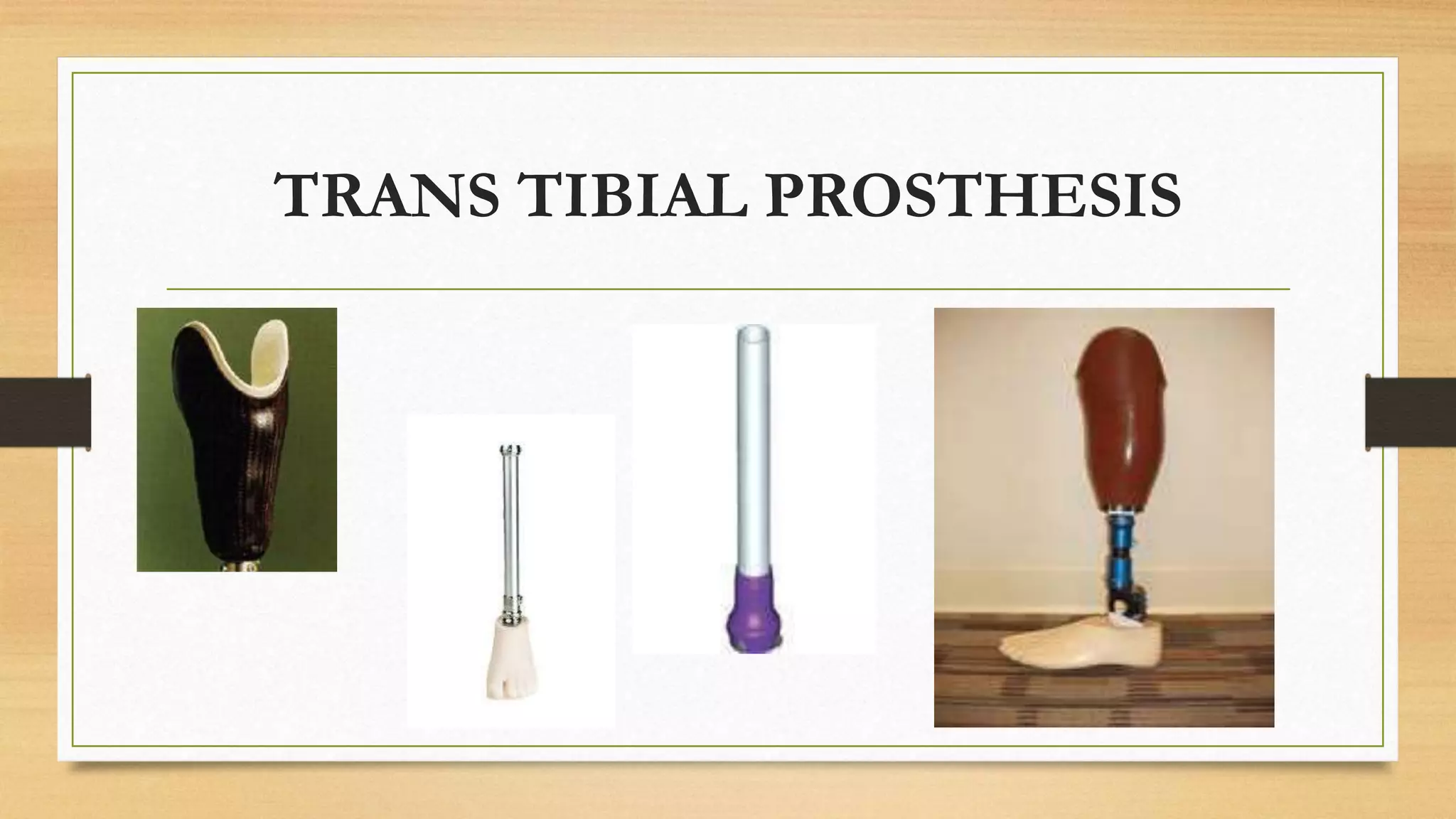
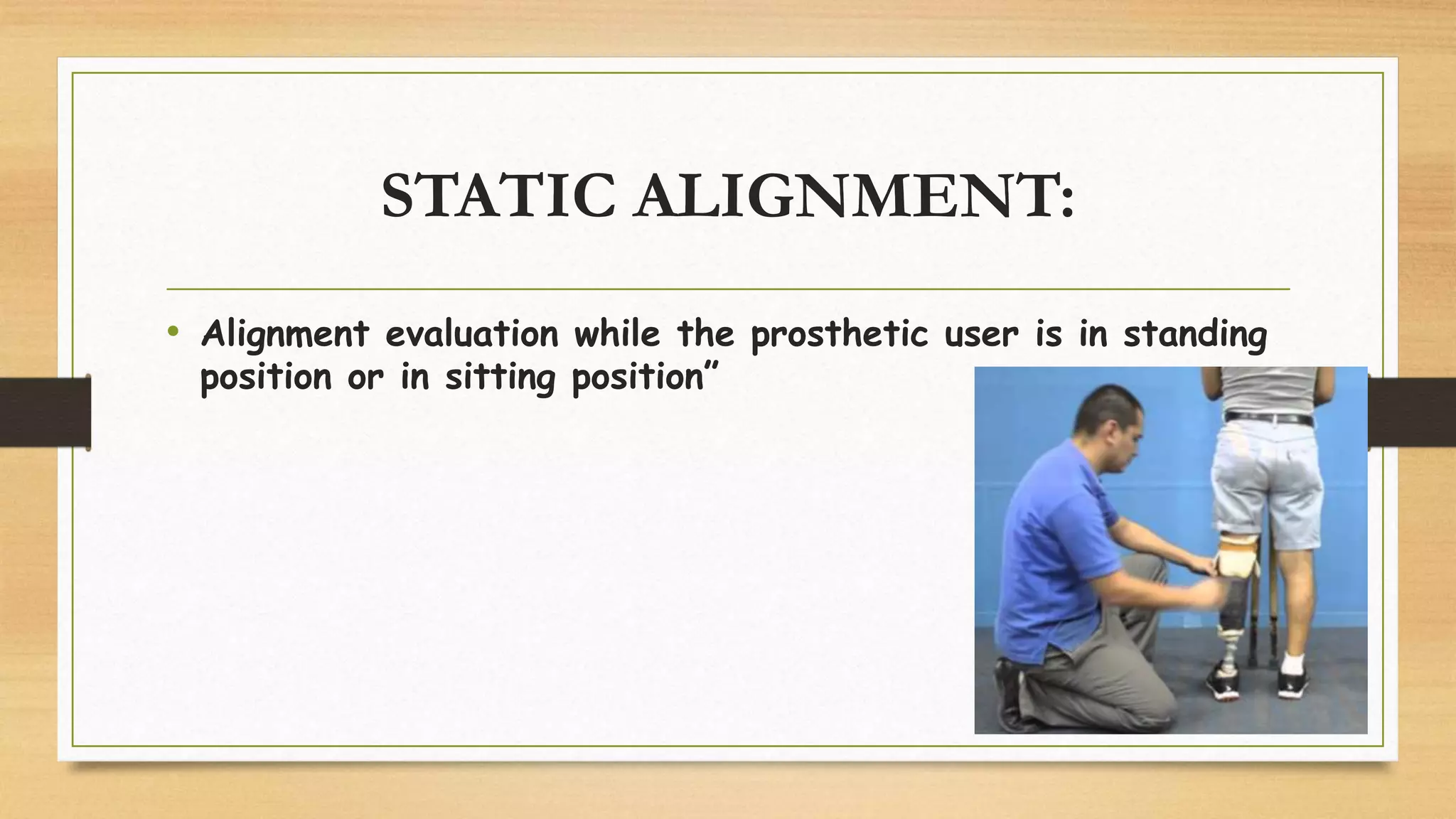
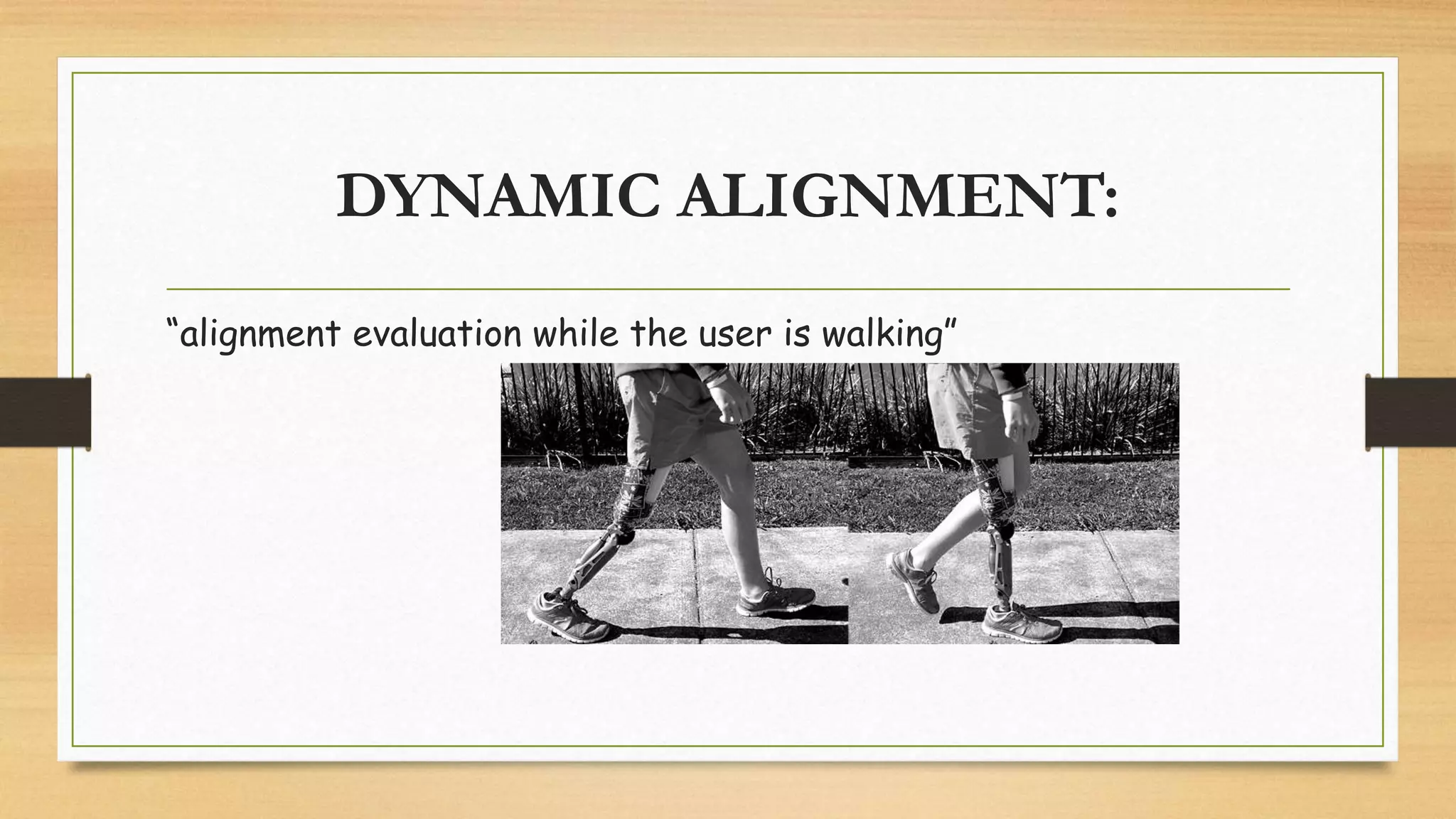
The document discusses the alignment of a trans-tibial prosthesis (TTP). It defines alignment as the spatial relationship between prosthetic components and the amputee's body. Proper alignment is important for comfort and a natural gait. There are three types of alignment discussed: bench, static, and dynamic. Bench alignment sets the initial positioning before fitting. Static alignment evaluates alignment while standing or sitting. Dynamic alignment observes the user walking to further refine the alignment based on gait analysis and user feedback. The goal is smooth, natural walking with even weight distribution and less energy expenditure.