Stable Angina Pectoris: Causes, Symptoms and Diagnosis
•
3 likes•633 views


Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Stable Angina Pectoris: Causes, Symptoms and Diagnosis
Similar to Stable Angina Pectoris: Causes, Symptoms and Diagnosis (20)
More from Alexandria University, Egypt
More from Alexandria University, Egypt (20)
Recently uploaded
Recently uploaded (20)
Stable Angina Pectoris: Causes, Symptoms and Diagnosis
- 1. Samir RaflaL: Principles of Cardiology pages 87-111 ISCHEMIC HEART DISEASE Disease of the coronary arteries is due to atherosclerosis in the majority of cases. However, the coronary arteries may be involved in other disorders as congenital abnormalities, coronary embolism, dissection, polyarteritis and coronary spasm. ATHEROSCLEROSIS Atherosclerosis consists of deposition of fatty substance rich in cholesterol in the subintimal layer of the arteries. Later, the intima overlaying the fatty deposition may fibrose resulting in fibrous cap. The covering fibrous cap may disrupt and an intimal ulcer occurs. The lumen of the vessel becomes progressively narrowed and finally complete obstruction occurs due to: 1. Progress of the narrowing. 2. Thrombosis over disrupted intimal plaque. 3. Hemorrhage in the subintimal region. PATHOGENESIS OF ATHEROSCLEROSIS: The response to injury hypothesis: It states that injurious agents e.g. hypertension and hypercholesterolemia cause endothelial damage. The injured endothelium becomes more permeable admitting cholesterol (specially the low density lipoprotein fraction) into the intima where it is oxidized and becomes cytotoxic. Macrophages from the blood and smooth muscle cells from the intima migrate into the lesion, proliferate, ingest the lipids, become foam cells and later rupture releasing their content in the interstitium and the cycle is repeated. Thus elements that play roles in atherosclerosis are: 1. Endothelium. 2. Monocytes/macrophages. 3. Smooth muscle cells. 4. Platelets. 5. Blood lipids. The mature plaque is composed of a lipid core that is covered by a fibrous cap. There are two types of plaques: 87
- 2. a. Stable plaques which have a small lipid core and a thick fibrous cap. It is not liable to rupture and thus unlikely to induce thrombus formation and acute occlusion of the artery. Unstable or Vulnerable plaques have a large lipid core and thin fibrous cap. It may be invaded by macrophages and inflammatory cells especially at its margins. These inflammatory cells secrete enzymes that digest the fibrous cap. The plaques are liable to rupture at their margins exposing the plaque core to the circulating blood. Platelets adhere to the exposed area and start a chain of platelet aggregation then coagulation cascade leading to an intravascular thrombus. This may reduce the vessel lumen or occlude it partly or totally. The diffusion of fats and cholesterol from the blood stream into the intima is accelerated by: 1. Increase in the concentration of cholesterol and other lipids. The normal total serum cholesterol is 150-190 mg%, but in persons with multiple other risk factors, diabetes or clinical coronary artery disease, this level should not exceed 175 mg%, Low-density lipoprotein cholesterol (LDL) is the major atherogenic lipid. LDL levels less than 130 mg% are considered desirable in otherwise normal persons. However, in persons with ischemic heart disease, diabetes or two or more risk factors the level of LDL should not exceed 100 mg%, reaching 70 mg% is now a desirable target. High-density lipoprotein fraction of cholesterol (HDL) is, in contrast, protective as is assists in the reverse transport of LDL from the cells back to the liver to be metabolized. The normal level of HDL in serum should be at least 40 mg% in males and 50 mg% in females. Triglycerides are less atherogenic but their level should not exceed 150 mg%. 2. Increase in the arterial blood pressure. Risk factors leading to atherosclerosis 1. Abdominal obesity, 2. Hypercholesterolemia, 3. Hypertension, 4. Diabetes and 5. Cigarette smoking are the most important risk factors leading to atherosclerosis. Additional risk factors are: 88
- 3. 6. Family history of ischemic heart disease (genetics). 7. Insulin resistance syndrome (metabolic syndrome). 8. Sedentary non-active life, 9. Mental and psychic stress. 10. Myxedema. PREVENTION OF ATHEROSCLEROSIS: Prevention of atherosclerosis is done by avoiding the above factors. Life style modification: by 1) Diet: The diet should be low ‘in fully saturated fats, cholesterol” 2) Walking 20 min daily 5 days per week. 3) Hypocholesterolemic drugs: The most important are: a. Statins i.e. HMG-CoA reductase inhibitors e.g. Simvastatin (Zocor, Atorvastatin (Lipitor), Fluvastatin (Lescol) and Rosuvastatin (Crestor). These are very effective in reducing cholesterol synthesis only. Side effects include rhabdomyolysis (i.e. skeletal muscle cell necrosis) and impaired liver function. b. Fibrate group of drugs e.g. gemfibrozil (Lopid), fenofibrate (Lipanthyl). c. Bile acid sequestrants e.g. Colestyramine (Questran) binds bile acids in the gut and prevents their reabsorption. d. Other drugs include fish oils, omega 3 fatty acids and ezetimibe (Ezetrol) (which inhibits cholesterol absorption in the gut). Combinations of ezetimibe and statins are used in severe cases and are very effective. 4) Treatment of underlying disease causing the increase in blood lipids, e.g. diabetes, myxedema, nephrosis, etc. 5) Treatment of hypertension. PRESENTATIONS OF ISCHEMIC HEART DISEASE STABLE ANGINA PECTORIS Definition: Angina pectoris is a discomfort in the chest and adjacent areas due to transiently inadequate blood supply to the heart. It is precipitated by effort and relieved by rest. ETIOLOGY: 89
- 4. Myocardial ischemia occurs when there is: A. Decrease in coronary blood flow due to: 1. Coronary atherosclerosis is the commonest cause. 2. Coronary artery spasm (Prinzmetal or variant angina). 3. Low cardiac output. 4. Severe lowering of the diastolic blood pressure, e.g. in aortic regurgitation. B. Excessive increase in cardiac work due to: 1. Severe hypertension. 2. Aortic stenosis. 3. Rapid tachycardia (tachycardia also shortens diastolic period during which the coronary arteries fill). 4. Hypertrophic myopathies. C. Reduction of oxygen carrying capacity of blood due to: 1. Severe anemia. CLINICAL FEATURES: The most characteristic feature is ischemic cardiac pain that is brought about by exertion and is relieved by rest. The pain fibers travel with the sympathetic nerves to the upper 4-5 thoracic spinal segments. That is why the pain is referred to the peripheral dermatomes supplied by these spinal segments. Character of cardiac pain: The pain is dull aching squeezing, compressing or burning of variable intensity. Instead of pain, angina may be perceived as compression, burning or even dyspnea on effort (angina equivalents). Site of pain: Cardiac pain is mostly substernal. It usually radiates to the left arm, sometimes it spreads to the root of neck, both shoulders and arms, back, epigastrium or the jaw. The pain may be felt only in the left arm or jaw. Relief: The pain forces the patient to stop and disappears after 1-3 minutes rest. Sometimes it lasts longer but not more than 15 minutes. It is also always relieved by sublingual nitroglycerine. 90
- 5. Associated manifestations: The pain may be associated with sweating, tachycardia, anxiety and rise in blood pressure. Some patients may have silent ischemia i.e. episodes of ischemia manifested by E.C.G. changes but without chest pain. This is particularly common in diabetics due to autonomic neuropathy. Silent ischemia is detected by the ECG during stress testing or during a 24 hour ambulatory E.C.G recording (Holter monitor). Precipitating factors include: 1. Effort is the most common precipitating factor, e.g. climbing stairs, running, walking, carrying heavy weight, etc. the pain occurs during effort. 2. Emotions. 3. Heavy meals. 4. Exposure to cold. 5. Sexual intercourse. 6. In severe cases pain may be precipitated by lying down i.e. angina of decubitus. Physical examination is usually free in between the attacks. During the attack a fourth heart sound may appear and a pansystolic murmur may be heard because ischemia of a papillary muscle may lead to ischemic mitral regurgitation. DIAGNOSIS AND INVESTIGATIONS: 1. History. 2. Exercise electrocardiography. 3. Radionuclide Perfusion Scintigraphy (Thallium study). 4. Multislice CT. 5. Coronary arteriography. This procedure is essential if the diagnosis is in doubt. It is also needed to help determine whether medical treatment, balloon angioplasty and stenting or surgery is most appropriate. Indications of coronary angio: in high risk patients such as: a. Patients not responding to medical treatment. b. Patients who develop chest pain or ECG changes on slight effort (highly positive exercise ECG). 91
- 6. c. Patients in whom the anginal pain is associated with dyspnea or hypotension. d. Patients who develop angina after an attack of myocardial infarction (post- Infarction angina). e. Those who develop the disease at young age e.g. below 40 years. f. Any patient over 40 years of age undergoing open-heart surgery for other purposes e.g. valve replacement. g. Patients resuscitated from sudden cardiac arrest. DIFFERENTIAL DIAGNOSIS: The following conditions cause pain that may simulate angina: 1. Anxiety and neurosis are perhaps the commonest and the most difficult differential diagnosis. 2. Esophageal spasm, reflux esophagitis and hiatus hernia. Here pain is related to meals but has no constant relationship to exertion. 3. Musculo-skeletal lesions, e.g. cervical or thoracic spondylosis, cervical rib, myositis, costochondritis (Tietz’e syndrome). 4. Cholecystitis. 5. Pleurisy and Pneumonia. 6. Pericarditis. 92
- 7. PROGNOSIS: The prognosis is variable depending on the status of left ventricular function, the number of the vessels involved as seen in coronary arteriography and on the presence of associated disease such as hypertension, heart failure, diabetes, myocardial infarction, arrhythmias, renal failure, etc TREATMENT: A. During the Attack: The most important drug is nitrates. They are used either as sublingual tablets e.g. isosorbide dinitrate (Isodril or Dinitra 5 mg) or nitroglycerine (Angised 0.3 mg), or as oral spray. They are coronary vasodilators but more importantly, they cause generalized decrease in arteriolar and venous tone. This reduces both the blood pressure and the venous return and thus lowers the oxygen demands of the heart. B. In Between Attack: The long-term management of angina consists of the following lines. 1. Improvement of Coronary Blood Supply: This is done by: a. Nitrates: b. Calcium channel blocker: improve angina by two mechanisms. i. They decrease or abolish spasm of coronary arteries. ii. They decrease myocardial contractility and thus decrease the myocardial oxygen demand. Either nifedipine or verapamil (Isoptin) or diltiazem can be used. c. Revascularization: This can be achieved either by surgery or by percutaneous trans-catheter angioplasty (PCI = Percutaneous Coronary Intervention). An operation has been devised to bypass the atherosclerotic obstruction in the coronary artery by a bypass graft (CABG) made of the saphenous vein, radial or internal mammary arteries. Dilatation of localized lesions can also be accomplished by a balloon catheter i.e. coronary angioplasty with deployment of a stent to keep the dilated segment widely open. Revascularization is indicated in all cases of severe angina not responding fully to medical treatment and in all cases of post infarction angina. 93
- 8. Surgical bypass grafting should be considered in: i. Patients with stenosis of the left main coronary artery exceeding 50% with or without symptoms. ii. Patients with significant obstruction (over 70%) in the three major coronary arteries especially in diabetics and those with LV dysfunction. On the other hand, percutaneous coronary intervention (PCI) with stenting should be considered in patients with localised lesions in one or two coronary arteries. PCI is successful in over 90% of cases. However, restenosis at the site of dilatation occurs within 6 months in about 15 – 20 %. New stents that elute a drug (the metal is covered with a drug) that decrease restenosis rate to 5- 10 % have been introduced (drug eluting Cypher and Taxus stents). Lesions that were previously considered unsuitable for PCI can often now be stented. These include: - Long coronary lesions (> 20 mm). - Total coronary occlusion. - Bifurcation lesions. - Vein graft stenoses. - Lesions of the left main stem. 2. Reduction of Myocardial Oxygen Needs: - Treatment of secondary factors that increase oxygen needs of the heart, e.g. hypertension, heart failure, tachycardias, thyrotoxicosis, etc. - Reduction of weight in obese patients. - Exercise training. This is called rehabilitation. Exercise may also help develop collaterals. - Avoidance of extreme emotions and treatment of anxiety by tranquilizers. - Beta-adrenergic blockers: They cause a decrease in myocardial oxygen consumption by the following mechanisms: Decrease the heart rate. Decrease the myocardial contractility. Decrease the blood pressure. 94
- 9. In patients with bronchospasm, diabetes, or peripheral vascular disease a cardioselective beta-blocker or beta and alpha blocker is preferred. - Stopping smoking. Nicotine predisposes to angina by: - Increases catecholamines. - Increases serum lipids. - Increases the heart rate and may precipitate arrhythmias. - Carbon monoxide in the smoke binds some hemoglobin as carboxyhemoglobin. - Avoiding situations leading to angina, e.g. walking after meals or in cold weather. 3. Prevention of Further Progression of Atherosclerosis. This is best done by avoiding factors predisposing to it i.e. hypertension, obesity, cigarette smoking and physical inactivity and by treating dyslipidemias (Statins for life). 4. Antiplatelet drugs e.g. aspirin 75-150 mg daily is used to prevent platelet aggregation and subsequent thrombosis in the narrowed vessel. SPASMODIC ANGINA: Angina can develop due to spasm of the coronary arteries. Spasm may occur in normal arteries but more commonly it occurs on top of coronary atherosclerosis. As the spasm is spontaneous, pain occurs in attacks not related to any precipitating cause and is relieved spontaneously. It occurs more commonly in the early morning after awakening the patient from sleep. It may be associated with arrhythmias. The attacks are associated with ST rise in the ECG instead of ST depression that occurs in classic angina. This is Variant or Prinzmetal angina. Attacks of coronary spasm respond to nitrates. However the best long-term prophylactic treatment is calcium channel blockers (amlodipine, diltiazem or verapamil). Myocardial ischemia and angina may occur also in patients with normal coronary arteries and without evidence of spasm. This condition probably results of disease of the microcirculation. It has been termed micro-vascular angina or syndrome X. Unstable Angina and Non-S-T Elevation Myocardial Infarction (NSTEMI) This term unstable angina is given to any of the following: a. When the severity, duration, or frequency of anginal attacks increase b. Moderate to severe angina of recent (< 1 month) onset. c. When angina appears on rest, or lying down. 95
- 10. d. Post-infarction angina. The ECG may be normal or may show S-T segment depression or T wave inversion beside any previous findings. Unstable angina and NSTEMI may start de nova or may develop on top of chronic stable angina. They develop when a break occurs in the fibrous cap covering an atherosclerotic plaque (plaque disruption). This leads to exposure of the lipids and other contents of the interior of the plaque to bloodstream. Platelet aggregation occurs on the raw surface and leads to the development of a non-occlusive thrombus that markedly diminishes (but does not totally obstructs) the lumen of the artery. Vasoactive substances released from the damaged endothelium and aggregated platelets leads to local coronary spasm. The condition may progress to complete occlusion and infarction or may heal. Treatment of unstable angina and NSTEMI: a. Hospitalization and bed rest. b. Anticoagulation by IV heparin or preferably by subcutaneous low molecular weight heparins (LMWH) e.g. enoxaparin (Clexan) I mg/kg every 12 hours. Nitroglycerine is given initially by IV drip and later by sublingual or oral route as long as anginal pain exists. c. Beta-blockers should be routinely added. d. Aspirin 150 mg should be immediately chewed in order to inhibit platelet aggregation then orally daily afterwards. e. Clopidogrel (Plavix, 75 mg) is a potent antiplatelet drug that should be added to aspirin. 4 tablets (300 mg) should be given initially followed by I tablet daily. f. When facilities exist, all cases of UA or NSTEMI who are at high risk should have coronary angiography done and, if the anatomy is suitable, should have coronary angioplasty (PCI) with stenting. High risk is considered present if: i. Pain persists over 20 minutes. iv. Elevated troponin level. ii. Hemodynamic instability occurs. v. Age over 70. iii. Progressive ECG changes. vi. Presence of diabetes. 96
- 11. vii. Previous MI or PCI. viii Presence of renal insufficiency. MYOCARDIAL INFARCTION INCIDENCE: Myocardial infarction is the commonest cause of death in adults in the world today. It is much more common in males between 40 and 70 years and is uncommon in females before menopause. ETIOLOGY: The vast majority of cases are due to coronary atherosclerosis. The predisposing factors for infarction and atherosclerosis are the same: d. Hypertension. e. Hypercholesterolemia. f. Positive family history g. Smoking h. Diabetes i. Lack of physical activity and excessive mental strain j. Obesity. PATHOLOGY: The basic mechanism underlying MI is disruption of an atherosclerotic plaque. The contents of the plaque are exposed to blood stream and platelets adhere to the ulcerated lesion. Further platelet aggregation follow and then a thrombus forms that totally occludes the artery. SITE: Infarction mostly involves the left ventricle and the ventricular septum. Right ventricular infarction is uncommon and always occurs as an extension of infarction involving the inferior surface of the left ventricle because the blood supply of both areas is usually derived from the same artery (the right coronary artery). The location and extent of infarction depend on the anatomic distribution of the vessel involved and the adequacy of collateral circulation. Thrombosis occurs most commonly in the anterior descending branch of the left coronary artery resulting in infarction of the anterior wall of the left ventricle and the septum (anteroseptal infarction). Occlusion of the circumflex artery produces anterolateral infarction. 97
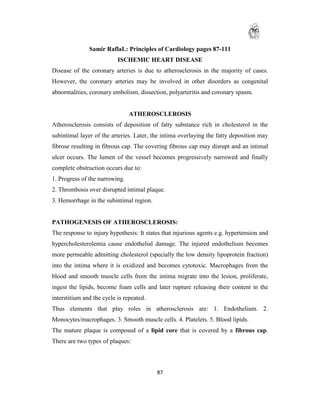
- 12. Obstruction of the right coronary artery leads to infarction of the postero-inferior part of the left ventricle and may involve the right ventricle. Fig: Anteroseptal MI. (A) One hour of onset of symptoms. (B) 12 h later. Infarction may involve the whole thickness of the myocardium i.e. transmural; or only the subendocardial region - nontransmural infarction). 98
- 13. Fig: Inferior myocardial infarction. (A) 1 h after the onset of symptoms. (B) Right sided chest leads recorded simultaneously. ST elevation is apparent in leads V3R to 99
- 14. V7R, indicating right ventricular infarction. (C) 12 h later. There are now deep Q waves in leads II, III and aVF. EFFECTS: - Part of the myocardium becomes necrotic. - If the area involved is very big, a very large part of the left ventricle will not share in the contraction resulting in a sudden severe drop in the cardiac output. Cardiogenic shock occurs. - Sudden death (sudden cardiac arrest within one hour of the symptoms) occurs in > 20 % of myocardial infarctions. - If the area involved is big left ventricular failure occurs and may lead to acute pulmonary edema. - The ischemic area around the infraction is always electrically unstable and is the site of genesis of many arrhythmias. - Ischemia or infraction may involve a papillary muscle. The mitral valve becomes unsupported and ischemic mitral regurgitation results. - The infracted area may rupture. If rupture occurs in the left ventricular free wall, hemopericardium and death occur. If the ventricular septum ruptures an acquired ventricular septal defect results. - When the visceral pericardium overlying the infarction is also involved it becomes roughened and pericarditis results. - When the endocardium is involved a mural thrombus may form over it in the left ventricle. Parts of the thrombus may detach later as systemic emboli. a. When the infarction heals it is replaced by fibrous tissue which may yield and expand gradually under the high intraventricular pressure resulting in a myocardial aneurysm. It leads to LV failure and cavity thrombus. CLINICAL PICTURE: Symptoms: 1) Cardiac pain: sudden onset of severe pain. It is of aching, burning or constricting character unrelated to exercise. The pain is maximal behind the sternum but may radiate to all the central part of the chest, neck, jaws, epigastrium, both shoulders, 100
- 15. specially the left, and the left arm. The pain is identical with that of angina in character, site and radiation but much more severe and prolonged and is not relieved by rest or by sublingual nitroglycerine. The pain may be preceded by recent onset of angina or sudden increase in its severity (crescendo angina). 2) Accompanying the pain there is usually profuse sweating, sometimes nausea and vomiting or syncope. Signs: d. Many patients have a sympathetic response leading to vasoconstriction, hypertension and tachycardia. Sometimes, especially in inferior infarction, there may be strong vagal reflexes with sinus bradycardia and hypotension. e. Cardiac examination is commonly normal but the fourth heart sound is usually present. The appearance of gallop rhythm, pericardial rub or systolic murmur indicates complications. Other manifestations: a. Fever. b. Leukocytosis. c. High erythrocyte sedimentation rate. Atypical Presentations: 1. Painless myocardial infarction occurs in the following situations: 2. Pain may be atypical in character site or radiation. 3. Presentation may be dominated by one of the complications, e.g. cases may present with shock, pulmonary edema, arrhythmias, etc. INVESTIGATIONS: I. Cardiac Enzymes: The most commonly used enzyme marker is creatinine kinase (CK) and its MB fraction (CK-MB). It starts to rise in the serum 4-6 hours after the onset of infarction, reaches peak value in 12 hours then starts to decline over 48-72 hours. CK-MB is cardio-specific while the total CK is not. Troponin (T or I), however, is the standard diagnostic enzyme test world-wide because it also has value in risk stratification. Its level correlates with the extent of myocardial damage and indicate the degree of risk. It also rises in 4-6 hours peaks in 101
- 16. 12 hours but disappears in 14 days, so that it is also of value in diagnosis of late cases. 2. Electrocardiography: The final proof of myocardial infarction is by the electrocardiogram. The classic evolution of changes is peaked (hyperacute) T waves, to ST segment elevation, to appearance of Q waves, to T wave inversion and return to ST segment to base line. This may occur over few hours to several days. However, Q waves may not appear in 30% of acute infarctions i.e. non-transmural or non-Q wave infarction. In these cases the infarction is subendocardial or consists of localized areas of necrosis within ischemic but viable myocardium. 3. Echocardiography: Echo will show hypokinesia or akinesia of the ischemic or necrotic ventricular wall. The overall left ventricular function can be estimated by the ejection fraction and it has a very important role in evaluating the immediate risk and the long-term prognosis of the patient. Two dimensional and Doppler echo are also very valuable in diagnosing complications such as ischemic mitral regurgitation, ventricular septal defect, myocardial aneurysm, pericardial effusion, etc. 4. Other laboratory findings include leukocytosis and high ESR. COMPLICATIONS: 1) Sudden Death: Occurs in 30% of acute MI in first month. 2) Arrhythmias: these are very common in the first few days after the infarction. They are the most common cause of death in the early stages. Nearly any arrhythmia can occur but the most common are: a. Ventricular extrasystoles occur in over 90% of cases. b. Ventricular tachycardia which causes marked circulatory deterioration. c. Ventricular fibrillation (VF) is fatal if untreated within minutes. Primary VF occurs very early and is caused by the onset of ischemia. Secondary VF occurs late and is usually secondary to heart failure, shock etc and indicate poor prognosis. 102
- 17. d. Atrial arrhythmias (e.g. extrasystoles, tachycardia, and fibrillation) are common when there is heart failure. 3) Left Ventricular Failure: results from extensive infarction and may present with dyspnea and orthopnea or, in severe cases, with acute pulmonary edema. On examination sinus tachycardia, a third heart sound or gallop rhythm and bilateral basal crepitations will be found. Right Ventricular Infarction is uncommon but may lead to right ventricular failure presenting with low cardiac output and high venous pressure. 3) Cardiogenic Shock: results from very extensive infarction. The cardiac output is very low. The patient is pale, cold, sweating and mentally dull with hypotension, peripheral cyanosis, oliguria or even anuria. When shock is severe the prognosis is very bad: mortality is over 80%. Shock may co-exist with left ventricular failure. 5) Conduction Defects: heart block may occur in the course of inferior infarction. This is because the right coronary artery usually supplies both the AV node and the inferior surface of the heart. In these cases the block is due to vagal reflexes or to transient ischemia of the A-V node and is usually transient and may respond to 103
- 18. atropine. If the bradycardia causes hemodynamic deterioration a temporary external pacemaker should be instituted to drive the heart at rate of 60/minute via a transvenous electrode catheter. Bundle branch block may occur. When this is associated with prolonged P-R interval it means that complete heart block may develop. 6) Mitral Regurgitation: is due to ischemia and fibrosis of a papillary muscle. Mild degrees of regurgitation are common. Rupture of a papillary muscle leads to very severe mitral regurgitation and intractable heart failure. 7) Pericarditis: when the pericardium is involved a pericardial rub is heard 2 to 3 days after the infarction and may lead to recurrence of pain. The pain of pericarditis must be differentiated ischemic cardiac pain that may be caused by extension of the infarction. Pericardial pain is increased with movements and inspiration. Hemorrhage in the pericardial sac (hemopericardium) may occur, especially if anticoagulants are used in the presence of pericarditis. 8) Emboli: embolism following myocardial infarction has many sources: a. When the endocardium is involved in the infarction, mural thrombi may form in the LV cavity and may lead to embolism in brain, other areas. b. In cases complicated by atrial fibrillation, thrombosis may form in the atria. 9) Myocardial Aneurysm: occurs after the healing stage and may lead to: a. Heart failure. b. Thrombosis and embolism. c. Diffuse or double apical impulse. 10) Rupture of the heart: may occur leading to hemopericardium, cardiac tamponade and sudden death. Rupture of the ventricular septum results in acquired ventricular septal defect. A pansystolic murmur appears at the lower left sternal edge. It may be associated with left ventricular failure and low cardiac output. 104
- 19. 11) Ventricular Remodeling: The healed myocardial infarction zone consists mainly of fibrous tissue that yields under the high intraventricular pressure resulting in infarct expansion. Other healthy areas of the myocardium hypertrophy in order to compensate for the areas of lost function. The ventricular cavity assumes a more globular form instead of the normal ovoid shape. These changes, taken together, are called ventricular remodeling and result in long-term deterioration of cardiac function and may ultimately end in left ventricular failure. 12) Depression, fear of death, and nervousness: Important complication to infarction. PROGNOSIS: If untreated, one fifth of cases of myocardial infarction die in the first few hours (sudden cardiac arrest). Another fifth die from various complications during the first month after infarction (these figures improved after advent of primary balloon angioplasty). Of those who recover 75% live 5 years and 50% for 10 years. Some may show post infarction angina pectoris. DIAGNOSIS: Myocardial infarction is diagnosed when there are two of the following: 1- Typical pain. 2- Typical ECG changes. 3- Enzyme rise. 4- Hypokinesia-akinesia by echocardiography. In typical cases the main diagnostic feature is ischemic cardiac pain associated with ST elevation of 1 mm or more in two contiguous ECG leads and elevated cardiac enzymes. However, the following diseases may simulate the cardiac pain of myocardial infarction. 1. Pulmonary embolism: When a main pulmonary artery is occluded the pain may simulate that of myocardial infarction. Dyspnea is the most common and outstanding symptom of pulmonary embolism. Enzymes CK, (MB), troponin and SGOT are normal and LDH is high. Electrocardiographic signs are different. If 105
- 20. pulmonary infraction occurs the pain is pleuritic, increases with inspiration and coughing and is associated with hemoptysis. D-Dimer enzyme rises in pulmonary infarction. 2. Acute pericarditis: 3. Dissecting aneurysm of the aorta: 4. Abdominal conditions: as acute indigestion, perforated peptic ulcer, biliary colic, acute cholecystitis, acute pancreatitis, hiatus hernia, esophagitis, etc... may simulate infarction. In these cases the pain is more epigastric and is accompanied by tenderness and rigidity over the affected viscous. The electrocardiogram and cardiac enzymes are normal. 5. Spontaneous pneumothorax produces pain that is usually unilateral with severe dyspnea. The X-ray is diagnostic and the ECG and the enzymes are normal. 6. Spinal and chest wall conditions like spondylitis, cervical disc, herpes zoster, pleurodynia etc. 7. Pneumonia and pleurisy. Treatment of S-T elevation myocardial infarction (STEMI): . Immediate treatment . Aspirin, Clopidogrel . Reperfusion therapy: - thrombolysis, - angioplasty PCI) . Beta-blockers, Angiotensin converting enzyme inhibitors. . Nitrates and other drugs. All cases of chest pain must be managed as an emergency. If the ECG show, elevation of the S-T segment of 1 mm or more in two contiguous leads, this must be considered a case of S-T elevation myocardial infarction (STEMI) and the patient should be rushed to hospital immediately. The primary aim of treatment is: a. Limit infarction size. b. Relieve symptoms. c. Prevent or treat complications. 106
- 21. 1) Coronary Care Units: The most common complications and cause of death in acute myocardial infarction are arrhythmias. In coronary care units, electric shock (i.e. defibrillation and cardioversion for ventricular fibrillation and tachycardia) and pacemakers (for heart block and cardiac arrest) are continuously available in addition to standard drugs. Resuscitation from cardiac arrest is most often required at this time. The most urgent measure is the relief of pain by IV morphine. If morphine is not available pethedine (50 mg) can be used. 2) Aspirin: A 300 mg tablet of aspirin (soluble or chewable) should be given as early as possible in acute infarction in order to reduce platelet aggregation at the site of atherosclerotic plaque.. Clopidogrel (Plavix) 4 (75 x 4 = 300 mg) tablets are given immediately also. 3) Reperfusion: By this is meant opening up of the occluded vessel so that blood can again perfuse the myocardium. It is the most important therapeutic measure and must be done as soon as possible. It is most useful when performed in the first 6 hours. Its value is doubted after 12 hours as by then necrosis of myocardium has already happened. It can be achieved in two ways: a. Thrombolytic or Fibrinolytic Agents: e.g. streptokinase, tissue plasminogen activators, and tenectaplase (TNK), etc, can dissolve coronary thrombus if they are administered within less than 6 hours of its formation. Reperfusion of the occluded artery is achieved in the majority of cases and infarction is reduced or prevented. 1.5 million l.U of streptokinase is usually given over a period of one hour by l.V. infusion. These drugs are indicated in every patient with infarction and with elevation of the S-T segment in two contiguous ECG leads (STEMI). Hemorrhage is the most important complication of fibrinolytic drugs. Contraindications to their use include bleeding diathesis, uncontrolled hypertension, recent internal bleeding, recent stroke, pregnancy, recent trauma or surgery and age above 80 years. b. Coronary angioplasty (Percutaneous Coronary Intervention PCI): 107
- 22. Balloon dilatation of the site of obstruction in the coronary arteries is probably the best method and it treats both the recent total occlusion and the underlying atherosclerotic plaque that led to it. If successful the ischemic zone is reperfused with blood and the myocardium at risk is salvaged. It can be used as the initial therapy (primary angioplasty) or when thrombolysis is contraindicated or has been used but failed. 4) Anticoagulant Drugs: Anticoagulation by unfractionated or low molecular weight heparin definitely decreases the risk of thrombosis in the deep veins of the leg and subsequent pulmonary embolism. They should be given during the acute phase when the patient is immobilized in bed for a long period e.g. in cases associated with heart failure, shock, or in patients with previous venous disease. 5) The use of beta blocking drugs is needed in patients with marked sympathetic overactivity presenting with sinus tachycardia without evidence of heart failure. The bradycardia resulting from beta blockade reduces the myocardial needs for oxygen and thus may help limit he infarction size. 6) ACE inhibitors: They have favorable impact on ventricular remodeling, improvements of hemodynamics and reduction in congestive heart failure. They proved to reduce death from AMI. 7) Nitrates: They reduce ventricular filling pressure, wall tension and cardiac work with improvement in coronary blood flow. 8) Physical Rest: Rest is essential until the infarct heals. Initially, it must be absolute except for the use of a bed-side commode. Rest period depends on severity and complications. In uncomplicated cases 1 week bed rest (arm chair allowed) followed by a period of restricted indoor activity. 9) Mental Rest: All patients must be given a tranquilizer to relieve anxiety. If necessary a sedative or hypnotic is given to help sleep. 10) Oxygen: Oxygen should be given specially if shock, left / ventricular failure or persistent chest pain is present. 108
- 23. Diet: During the first few weeks diet must be: Low calorie, low salt, light, and easily digestible. Smoking: Smoking must be completely forbidden during the acute phase and preferably for life afterwards. Treatment of complications: Heart failure is treated by diuretics, vasodilators and positive inotropic agents e.g. dobutamine. Digoxin is not recommended in acute myocardial infarction except to control the ventricular response in rapid atrial fibrillation. Pulmonary edema by intravenous morphine, IV frusemide, positive inotropic drugs, oxygen, aminophylline, and vasodilators. Cardiogenic shock: The usual first aid measures are warmth, oxygen, relieve of pain, and raising the foot of the bed. Other measures that are useful may include: a. Drugs that increase myocardial contractility e.g. dopamine dobutamine. At low loses (2-4 mg/kg/mm) dopamine improves the renal blood flow. At intermediate doses (2.5-10 mg/kg/mm) it stimulates the myocardial contractility. At higher doses it is a potent vasoconstrictor. b. Fluids in cases with hypovolemia, due to sweating, vomiting and lack of fluid intake. c. Vasoconstrictors as noradrenaline are used if above measures fail. d, Coronary angioplasty is the best treatment of cardiogenic shock after MI. f. When shock is due to the presence of severe ischemic mitral regurgitation or ventricular septal defect, then emergency surgery must be done to correct the cause. g. If the above measures fail the patient is stabilized by assisted circulation. A balloon tipped catheter is introduced from the formal artery to the descending aorta and inflated mechanically during every diastole. This is intra-aortic balloon counterpulsation. It partly relieves the heart and maintains blood flow in diastole until the myocardium recovers. Ventricular extrasystoles (if frequent) are best treated by lignocaine IV bolus or drip. Other oral drugs such as amiodarone can be used for oral prophylaxis against recurrent arrhythmia. 109
- 24. Ventricular tachycardia is best treated by electric shock (cardioversion). If this is not available intravenous lignocaine or amiodarone or procainamide can be used. Ventricular fibrillation causes complete cessation of the circulation. Life is sustained by immediate cardiac massage and artificial respiration. Defibrillation by electric shock causes the return of sinus rhythm. Ventricular aneurysm may result in refractory heart failure and recurrent emboli. It can be excised surgically. Heart block is treated by atropine and temporary external pacemaker. Sinus bradycardia should be treated with atropine. Long Term Management: As in angina pectoris, the management includes: 1. Increase in myocardial oxygen supply by coronary vasodilators and exercise, which promotes formation of collaterals. 2. Reduction of myocardial oxygen needs by reduction of weight, sedation and beta- adrenergic blockers. The long-term use of beta- blockers has definitely been shown to reduce the mortality and the incidence of re-infarction. 3. Prevention of expansion of the area of infarction and progressive development of heart failure (ventricular remodeling) by the use of angiotensin converting enzyme (ACE) inhibitors on long term basis. They should be started from the first week after large infarction and continued indefinitely. 4. Prevention of further progression of atherosclerosis. 5. Long-term anticoagulants: The majority of cardiologists today tend not to use anticoagulants at all or to discontinue them gradually as the patient returns to full activity. 6. If angina persists after the infarction (post-infarction angina) the patient must be subjected to coronary arteriography to delineate the extent of coronary arterial lesions and decide the need for surgery or balloon-angioplasty. 110
- 25. 7. Rehabilitation: Graduated activity with increasing exercise is now considered the major factor in increasing physical fitness and allowing more work to be done with the least oxygen needs. ANTICOAGULANTS HEPARIN: Two forms of heparin exist: unfractionated heparin (UFH) and low molecular weight heparin (LMWH). UFH is given by the IV route starting with a loading dose of 5000 to 10000 units mg then continued either by IV infusion of 1000 U/hour or by intermittent injection of 5000 U/4 hours. It combines in the body with antithrombin III and acts both on activated factor II (thrombin) factor X. LMWH act primarily on factor X. They do not need laboratory monitoring. They are given subcutaneously every 12 hours. Eg enoxaparin (Clexan). ORAL ANTICOAGULANTS: These drugs act by inhibiting the synthesis of prothrombin in the liver. They do not affect already circulating prothrombin. That is why their action is delayed for about 48 hours and persists 48 hours after their withdrawal until new prothrombin is formed. GENERAL INDICATIONS OF ANTICOAGULANTS: 1. Pulmonary embolism. 2. Deep vein thrombosis. 3. Atrial fibrillation. 4. Arterial embolism and thrombosis. 5. Some cases of myocardial infarction e.g. those associated with ventricular aneurysm or left ventricular cavitary thrombus. GENERAL CONTRA-INDICATIONS OF ANTICOAGULANTS: 1. All conditions predisposing to hemorrhage, e.g. recent surgery, peptic ulcer, open ulcers, gastrointestinal bleeding, etc... 2. In pericarditis to avoid (hemopericardium). 3. In infective endocarditis. 4. In severe hypertension. ANTI PLATELET DRUGS 1. Aspirin 75-160 mg daily is the most effective and most widely used. 2. Clopidogrel (Plavix, Stroka, 75 mg). Inhibit ADP action on platelet receptors. 111
- 26. 3. The IIb IIIa receptor blockers: are the most potent but can be given only by IV infusion and are used in patients with acute coronary syndrome who will undergo coronary angioplasty. E.g. tirofiban (Aggrastat). 4. Dipyridamole (Persantin, 75 mg t.i.d.) is rarely used now. 112