
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hiatus hernia
Similar to Hiatus hernia (20)
Recently uploaded
Recently uploaded (20)
Hiatus hernia
- 1. HIATUS HERNIA under the guidance of Dr.M.Anand MS.FRCS. Dr.A.Suvarchala MS. Dr.TVSS.Nagababu MS. Dr.Venkatnaidu MS.
- 2. • It is a type of hernia characterised by protrusion of abdominal organs especially stomach into chest cavity through the oesophageal hiatus (T10) of the diaphragm
- 3. RISK FACTORS • Most common – obesity old age • Others: major trauma scoliosis
- 4. ETIOLOGY • Increased intra abdominal pressure – • heavy lifting • frequent/hard coughing • violent vomiting • straining during defecation • Trauma to the diaphragm • Congenital anomalies
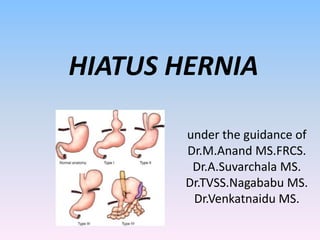
- 5. • Type 1 / sliding hiatus hernia : • Upward displacement of GE junction into posterior mediastinum • Stomach remains in its usual longitudinal alignment • Prevalence and size correlate with severity of reflux disease.
- 6. • Type 2 / true PEH/rolling hernia: • Normally positioned intraabdominal GE junction with upward herniation of the stomach alongside it. • Develops when there is a defect possibly congenital in the hiatus anterior to oesophagus • Angle of his is maintained
- 7. • Type 3/ Mixed hernia: • Displacement of both the GE junction and a large portion of stomach cephalad into posterior mediastinum
- 8. • Starts as a sliding HH and over time as hiatus enlarges and more of fundus and body of stomach herniate into chest
- 9. • Type 4 hernia: • Hernia sac also contains other organs such as the spleen , colon , or small bowel.
- 10. PATHOPHYSIOLOGY • Widening of the diaphragmatic crura at oesophageal hiatus • Stretching of phrenooesophageal membrane • As the hernia enlarges phrenoesophageal membrane balloons into posterior mediastinum like a parachute. • Adhesions develop between wall of sac and surrounding structures
- 11. • Most common organ to herniate is the fundus of stomach • However entire stomach , spleen ,colon,pancreas, small bowel and omentum can migrate. • Gastric volvulus develops because of laxity in stomach’s peritoneal attachments and subsequent rotation of gastric fundus • on organoaxial or mesenteric axis • Risk of acute strangulation -1% per year
- 12. CLINICAL FEATURES • type 1- most common – GERD • Paraoesophageal hernias: -Most common- gastroesophageal obstructive symptoms – - Dysphagia, odynophagia , early satiety • Intermittent epigastric, chest pain secondary to visceral torsion and distension leading to ischemia of contents
- 13. • TYPE 2: most dangerous- • mucosal ischemia - gastrointestinal bleeding • -perforation • Ulceration of gastric mucosa- CAMERON’S ULCER – vertical riding ulcer • Respiratory symptoms – SOB by mass effect of hernia (type 3,4)
- 14. INVESTIGATIONS: • IOC: CT thorax with upper abdomen (oral contrast) • Others: • Barium oesophagogram • Upper GI endoscopy • Manometry • Ambulatory pH monitoring
- 17. TREATMENT • Type 1: • Medical: 1. modifying lifestyle factors, stop somking 2. Antacids,PPI 3. Domperidone,metoclopromide,erythromycin • Surgical: Elective Nissen fundoplication
- 19. • Operative repair of PEH: 1. THORACIC 2. ABDOMINAL • Open • laparoscopic
- 21. Key steps: 1. Reduction of hernia contents into abdominal cavity by gentle traction 2. Left triangular ligament, gastrohepatic ligaments ,phreno oesophageal ligaments cut 3. Divide gastrophrenic ligament and short gastric vessels to to mobilise fundus and expose left crus. 4. Complete excision of hernia sac from posterior mediastinum
- 22. Most challenging – mobilising posterior sac • Oesophagus and posterior vagus are closely associated with sac posteriorly • Pleura ,pericardium,aorta,inferior pulmonary veins are closely associated with sac • After sac is freed at hiatus an effort is made to remove as much of hernia sac from mediastinum as possible
- 23. 4. Mobilisation of distal oesophagus to achieve a minimum 3 cm of intra abdominal oesophagus length 5.The crura are reapproximated tension free with interrupted non absorbable suture if not possible- • Close the hiatus under tension+reinforce with biologic mesh • Diaphragmatic relaxing incision + reinforce with biological mesh
- 25. • 5. An antireflux operation - • Severely ineffective motility /apersitaltic oesophagus- TOUPET fundoplication • Rest others- NISSEN fundoplication
- 26. Complications: • Dysphagia – 3 weeks – mucosal oedema • If more than 3 weeks – tight wrap, tight hiatus closure , missed other motility disorders • Gas bloat syndrome • Disruption • Slippage • Perforation • Rare- injury to spleen(1-5%),vagi, pneumothorax .
- 27. References: • Sabiston textbook of surgery • Bailey and love 27th edition • Srb surgical operations text and atlas • internet
- 28. THANK YOU…