
Recommended
More Related Content
What's hot
What's hot (20)
Similar to renal stones pathophysiology
Similar to renal stones pathophysiology (20)
Recently uploaded
Recently uploaded (20)
renal stones pathophysiology
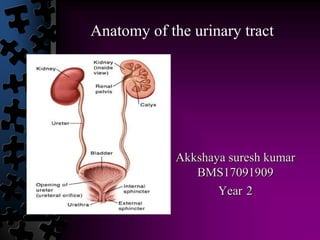
- 1. Akkshaya suresh kumar BMS17091909 Year 2 Anatomy of the urinary tract
- 2. • Text Anterior relations : LR
- 4. ● Text BLOOD SUPPLY TO THE KIDNEY
- 5. TEXT CONSTRICTIONS 1. Ureteropelvic junction 2. Pelvic inlet 3. Uretrovesical junction URETER :‣ 25 - 30 cm length and 3-4 mm in diameter ‣ descends on top of the psoas major muscles.
- 6. ● Text ‣ In the abdominal region ,apart from the renal artery ,the branches from gonadal artery ,the aorta ,and common iliac artery anastomose with each other . ‣ During operations , in the posterior abdominal region , surgeons pay special attention to the location of the ureter and their blood supply and are careful not to retract them unnecessarily . TO THE URETER,
- 7. ● Text‣ As they cross the pelvic brim , the ureters are in very close proximity to the ovaries. ‣ Approximately ,2cm above the ischial spine , the ureters run underneath the uterine artery . ‣ In male , instead of uterine artery ,the vas deferens cross the ureter anteriorly . CLINICAL IMPORTANCE :
- 8. Urinary bladder : ‣ Located anteriorly in the pelvic cavity , just posterior to the pubic bone . ‣ Trigone is a smooth triangular area between the opening of the ureter and the urethra on the inside the bladder .
- 9. TEXT RELATIONS : AT THE BASE : SUPERIOR SURFACE : ANTERIOR SURFACE : ( Inferolateral ) ‣ Retropubic space ‣ Puboprostatic ligaments ‣ Obuturator internus and Levator ani APEX : ‣ Median umbilical ligament . ‣ Rectovesical pouch in the male ‣ Vesico uterine pouch in female ‣ Peritoneal cavity containing loops of ileum ‣ Sigmoid colon ‣ Uterine cervix
- 10. ● Text TO THE BLADDER ,
- 11. • Text Innervation ‣ T11 -L2 nerves ‣ Contraction of the internal sphincter ‣ Inhibitory to the detrusor muscle SYMPATHETIC : PARASYMPATHETIC : ‣ S2 -S4 ‣ Pelvic splanchnic nerves , inf. Hypogastric nerve plexus . ‣ Motor of detrusor muscle ,inhibitory to the internal urethral sphincter in males . SOMATIC AND PUDENDAL NERVES : ‣ S2- S4 ‣ Innervates the external urethral sphincter (voluntary )
- 12. TEXT SPHINCTERS IN URETHRA: Sphincter vesicae : ‣ Surrounds the internal urethral orifice . ‣ Supplied by sympathetic fibres from T11— L2. Sphincter urethrae : ‣ Surrounds the membranous part of the urethra . ‣ Supplied by pudendal nerve from S2, S3 and S4.
- 13. THANK YOU REFERENCE : • GRAY’S ANATOMY • Clinical anatomy , Richard S. Snell , Edition 9 • https://www.earthslab.com/anatomy/kidneys/#content-location • https://teachmeanatomy.info/abdomen/viscera/kidney/ • https://teachmeanatomy.info/pelvis/viscera/urethra/
- 14. Pathophysiology of renal stones Sirajuddin Raeesah Firdhouse BMS17091830 Year 2
- 15. Renal stones Renal stones are polycrystalline structures that form from components of urine. The development of kidney stones is influenced by the concentration of stone components in the urine , the ability of the stone components to complex and form stones , and the presence of substances that inhibit stone formation. Stones require a nidus to form and a urinary environment that supports continued crystallization of stone components.
- 16. Aetiopathogenesis • Increased blood or urinary levels of stone components Interactions among the components Anatomic changes in urinary tract structures Metabolic and endocrine influences Dietary and intestinal absorption factors Urinary tract infection
- 17. Types of renal stones Calcium oxalate monohydrate Calcium phosphate Uric acid Struvite stone Cysteine
- 18. Composition and contributing factors to renal stones Type of stone Contributing factors Calcium ( oxalate and phosphate) Hypercalcemia and hypercalciuria, hyperparathyroidism, intestinal bypass surgery. Magnesium ammonium phosphate (struvite) Urea splitting urinary tract infection Uric acid ( urate ) Formed in acid urine with pH of approx 5.5, gout , high purine diet , Cystine Cystinuria ( inherited disorder of amino acid metabolism )
- 19. Pathophysiology of real stone formation • Stasis of urine flow predisposes to supersaturation of the urine with the particular element that first become crystallized and then become stones. • Damage to the lining of the urinary tract. • Decreased inhibitor substance in urine which would otherwise prevent supersaturation and crystalline aggregation.
- 20. Pathophysiology of renal stone formation
- 21. Pathogenesis of stone formation Stone formation Crystal growth and aggregation Crystals inter-reaction Crystallization, nucleation, growth and aggregation Urinary supersaturation Supersaturation depends on urinary pH, solute concentration, ionic strength, and complexation. More the ions , more risk of stone formation Stasis of urine flow Predisposing factor for renal damage
- 22. Pathology Mechanical obstruction of urine outflow results in : Increased backflow pressure into the kidneys Progressive hyperactivity and hypertrophy Progressive dilatation of renal calyces and pelvis Muscular loss of peristaltic activity leading to; stagnation of urine, increased risk of infection , increased risk of formation of stones. Progressive atrophy of renal parenchyma Induce non-infective inflammation in interstitial tissue of the kidneys. Compression of the arcuate artery leading to ischemic atrophy. The effects depend on either the obstruction is unilateral or bilateral.
- 23. Microbiological aspect of renal stones
- 24. Urolithogenic organisms. • Urea splitting organisms: • Proteus providentia • Staphylococcus aureus • Klebsiella • Pseudomonas • Mycoplasma Urea splitting organisms result in excessive production of ammonia and urinary alkalization leading to the formation of STRUVITE STONES ( magnesium ammonium phosphate stones .
- 25. Urea splitting organisms Proteus, Pseudomonas, Klebsiella,Mycoplasma
- 27. References. • https://en.wikipedia.org/wiki/Struvite • https://www.slideshare.net/reebababythomas/re nal-calculi-ppt • Harrisons principles of internal medicine • Robbins and cotrans pathology • Essentials of pathophysiology- Carol Matttson Porth •
- 28. Biochemistry of renal calculi Abdun Nafay Year 2
- 29. Type to enter a caption.
- 30. 1. Calcium stones •Consist of >90% oxalate with trace amounts of phosphate. •An estimated 40–60% of all calcium stone formers have hypercalciuria. •Occur primarily in individuals who excrete excess levels of oxalate in urine. •Primary hyperoxaluria, a rare autosomal recessive condition, causes disturbances in the oxalate biosynthetic pathway, leading to very high oxalate excretion
- 33. 3. Uric acid stones : • Uric acid (UA) is an end product of purine metabolism that the body excretes in urine. • Both purine overproduction and excess purine ingestion favor formation of UA stones. • The three major risk factors for UA stones are low urine pH (<5.5), low urine volume, and hyperuricosuria.
- 35. Uric acid stones
- 36. 4. Struvite stones : • Struvite stones consist of a mixture of magnesium, ammonium, and phosphate • Bacteria (Proteus, Staphylococcus, Klebsiella, and Pseudomonas) hydrolyse urea to produce NH4+ and OH– ions that contribute to the alkalinity of urine. • Both ammonium and alkaline urine are essential for struvite supersaturation of urine.
- 37. Struvite stones
- 38. 5. Cystine stones : • Mutations in two genes, SLC3A1 and SLC7A9 cystinuria • Because cystine has limited solubility, increased levels in urine favor its precipitation and contribute to formation of cystine stones excrete increased amounts of urinary cystine.
- 39. Cystine stones
- 41. Clinical manifestations of urolithiasis Hajira Shahid Year 2
- 42. Clinical manifestations ● May be asymptomatic ● Severe renal colic and abdominal pain. ● Larger stones often manifest themselves by hematuria. ● Nausea/ vomiting ● Loin pain occurs - can be dull or sharp, constant or intermittent. ● Complete anuria - suggestive of complete bilateral obstruction. ● Polyuria (may occur in partial obstruction) ● Infection may lead to malaise, fever and septicemia.
- 43. Symptoms of bladder outflow obstruction ● Symptoms may be minimal. ● Diminished force of urinary stream, terminal dribbling and sense of incomplete bladder emptying. ● Infection commonly occurs causing- a. Increased frequency b. Urgency c. Incontinence d. Dysuria e. Passage of cloudy, smelly urine.
- 44. Complications ● Serious infection of the kidney diminishes renal function ● Urinary fistula formation ● Ureteral scarring and stenosis ● Ureteral perforation ● Urinary outflow obstruction : hydronephrosis - chronic renal failure.
- 46. Workup
- 47. References ● Kumar and Clark Clinical Medicine 8th Edition ● Harrison Manual of Medicine 19th Edition ● Davidson’s Essentials of Clinical Medicine ● https://emedicine.medscape.com/article/437096-clinical ● https://www.mayoclinic.org/diseases-conditions/kidney-stones/symptoms-causes/syc- 20355755 Thank you