Tonsilitis
•Download as PPTX, PDF•
2 likes•983 views

tonsilitis : it's causes, sign and symptoms, nursing management

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Tonsilitis
Similar to Tonsilitis (20)
More from government hospital
More from government hospital (20)
Recently uploaded
Recently uploaded (20)
Tonsilitis
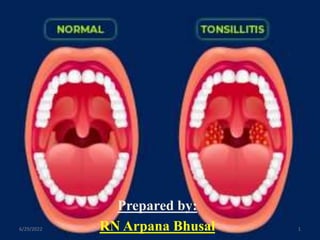
- 1. Prepared by: RN Arpana Bhusal 6/29/2022 1
- 2. 6/29/2022 2
- 3. CONTENTS Anatomy Introduction Causes Pathophysiology Classification Sign and symptoms Diagnostic evaluation 6/29/2022 3
- 5. 6/29/2022 5
- 6. ANATOMY The tonsils are 3 masses of tissue: Lingual tonsil Pharyngeal (adenoid) tonsil Palatine or fascial tonsil Together they form Waldeyer's ring Are lymphoid tissue Covered by respiratory epithelium Pseudostratified ciliated Columnar epithelium 6/29/2022 6
- 9. Anatomy cnt… Produce lymphocytes Are active in the synthesis of immunoglobulins. Generally, the palatine tonsils referred to as “the tonsils”. 6/29/2022 9
- 10. Introduction Tonsillitis is inflammation of the tonsils most commonly caused by a viral or bacterial infection. That can be acute, sub-acute, and chronic due to causative factors affecting it. 6/29/2022 10
- 11. 6/29/2022 11
- 12. CAUSES Bacterial and viral infections can cause tonsillitis through droplet infection. A common cause is Streptococcus bacteria. Other common causes include: Adenoviruses Influenza virus Epstein-Barr virus Parainfluenza viruses Enteroviruses Herpes simplex virus 6/29/2022 12
- 13. 6/29/2022 13
- 14. Predisposing factors Endogenous URTI Postnasal discharge due to sinusitis Residual tonsillar tissue after tonsillectomy Exanthemata Blood dyscrasias 6/29/2022 14
- 15. Predisposing factors cnt… Exogenous Cold drinks and foods Contact with infected persons Crowded and ill-ventilated environment Imbedded foreign body 6/29/2022 15
- 17. Classification Acute tonsillitis Sub-acute tonsillitis Chronic tonsillitis 6/29/2022 17
- 18. Acute tonsillitis Acute tonsillitis tends to be bacterial or viral in nature. Acute infection of the tonsils involving the surface epithelium, crypts and lymphoid tissue This is the commonest URTI in children. Occurs up to the age of 15; common in all sexes Incubation period ; is 72 hours. Viral: HSV, EBV,CMV, Adenovirus, Measles. Bacteral: anaerobes, group A beta hemolytic strepto pyogens, mycoplasma, chlamydia, N.gonorrhea 6/29/2022 18
- 19. Acute Tonsillitis subtype I. Acute superficial/catarrhal tonsillitis II. Acute membranous tonsillitis III. Acute follicular tonsillitis IV.Acute parenchymatous tonsillitis 6/29/2022 19
- 20. i. Acute catarrhal/superficial Here tonsillitis is a part of generalized pharyngitis, mostly seen in viral infections 6/29/2022 20
- 21. ii. Acute membranous Follows stage of acute follicular tonsillitis where exudates coalesce to form membrane on the surface 6/29/2022 21
- 22. iii. Acute follicular Infection spread into the crypts with purulent material, presenting at the opening of crypts as yellow spots. 6/29/2022 22
- 23. iv. Acute parenchymatous Tonsil in uniformly enlarged and congested 6/29/2022 23
- 24. 6/29/2022 24
- 25. Symptoms and Signs Symptoms: Sore throat – raw sensation in the throat Refusal to eat due to odynophagia Earache – either referred pain from the tonsil or due to acute otitis media Voice becomes thick and muffled Fever, may be associated with chills and rigor. Headache 6/29/2022 25
- 26. Signs cnt… Signs: 1. Tonsils appear congested and swollen Yellowish spots – follicular Whitish membrane – membranous Red and enlarged – parenchymatous 2. Hyperemia of pillars, uvula, soft palate 3.Halitosis, impeded movements of palate and increased secretions 4.Enlarged and tender jugulodigastric nodes 6/29/2022 26
- 27. Chronic Tonsillitis Characterized by recurrent acute attacks. It lasts between 3 weeks to 3 month in duration. Incubation period ; is 4-6 days . Etiology: 1. Recurrent acute tonsillitis 2. Subclinical infection of tonsils 3. Chronic infection in sinuses or teeth. 4. Complication of acute tonsillitis 6/29/2022 27
- 28. Symptoms and Signs Symptoms: Recurrent throat pain Cough Halitosis and bad taste in the mouth Quiescent phase: discomfort, irritation, pain; asymptomatic 6/29/2022 28
- 29. Signs: Chronic parenchymatous :- Appearance: hypertrophied, congested chronic follicular; small, fibrotic with cheesy debris. Squeezing: pus oozes out – should be distinguished from lymphatic fluid of normal tonsils 6/29/2022 29
- 30. Retention cysts: yellowish swellings filled with yellow liquid and debris Enlarged jugulodigastric nodes 6/29/2022 30
- 32. Diagnostic evaluation Clinical presentation 1.HISTORY Individuals with acute tonsillitis present with fever, sore throat, foul breath, dysphagia, odynophagia and tender cervical lymph nodes. Airway obstruction may manifest as mouth breathing, snoring, sleep-disordered breathing, nocturnal breathing pauses, or sleep apnea. 6/29/2022 32
- 33. Diagnosis cnt… Lethargy and malaise are common. Symptoms usually resolve in 3-4 days but may last up to 2 weeks despite adequate therapy. Recurrent streptococcal tonsillitis is diagnosed when an individual has • 7 culture-proven episodes in 1 year, • 5 infections in 2 consecutive years, or • 3 infections each year for 3 years consecutively 6/29/2022 33
- 34. Diagnosis cnt… Individuals with chronic tonsillitis may present with chronic sore throat, halitosis, tonsillitis, and persistent tender cervical nodes. Children are most susceptible to infection by those in the carrier state. Individuals with peritonsillar abscess (PTA) present with severe throat pain, fever, drooling, foul breath, trismus (difficulty opening the mouth), and altered voice quality (the hot-potato voice). 6/29/2022 34
- 35. Diagnosis cnt… 2. PHYSICAL EXAM Should begin by determining the degree of distress regarding airways and swallowing. Examination of pharynx may be facilitated by mouth opening without tongue protrusion, followed by gentle central depression of the tongue. Full assessment of oral mucosa, dentation, and salivary ducts may then be performed by gently “walking ”a tongue depressor about the lateral oral cavity. 6/29/2022 35
- 36. Diagnosis cnt… Acute tonsillitis reveals fever and enlarged inflammed tonsil that may have exudates. Open mouth breathing and voice changes result from obstructive tonsillar enlargement. Voice change in acute tonsillitis is not as severe as that with peritonsillar abscess 6/29/2022 36
- 38. 6/29/2022 38
- 39. Diagnosis cnt… 3. INVESTIGATIONS Testing is indicated when group A beta-hemolytic Streptococcus pyogenes (GABHS) infection is suspected. Throat cultures (sensitivity 90-95%) are the criterion standard for detecting GABHS. Lab Studies Complete blood count for elevated white blood cells & lymphocytes 6/29/2022 39
- 40. Diagnosis cnt… Imaging Peritonsillar abscess CT scan with contrast is indicated in general for unusual presentation(e.g. inferior pole abscess) and for pts at high risk of drainage procedures. For patients in whom acute tonsillitis is suspected to have spread to deep neck structures radiologic imaging using plain films of the lateral neck or CT scans with contrast is warranted. 6/29/2022 40
- 41. MANAGEMENT 1. Medical management Corticosteroids(shorten the duration of fever and pharyngitis. Antibiotics(oral penicillin and erythromycin; for 7 to 10days), IM for non compliant patient of oral therapy. Analgesics, Antipyretics Symptomatic treatment Treatment of co-existing infection of teeth, sinus and nose. 6/29/2022 41
- 42. 2. Supportive care Bed rest Soft diet Plenty of fluids Warm saline gargles Ice compression as PRN Provide communication pads Anticipate patient needs instead of asking Maintain air humidification 6/29/2022 42
- 43. Surgical management TONSILlECTOMY INDICATIONS FOR TONSILLECTOMY The American Academy of Otolaryngology– Head and Neck Surgery (AAO-HNS): Enlarged tonsils that cause upper airway obstruction, severe dysphagia, sleep disorders Recurrent peritonsillar abscess. Recurrent acute tonsillitis: attack occurring 4-6 times per year or more despite adequate medical therapy(i.e. antibiotics) and that is affecting quality and lifestyle (work/school) of the patient. 6/29/2022 43
- 44. Indication cnt… Obstructive sleep apnea: when large tonsils physically block the passage of the airflow causing snoring pauses in breathing during sleep, lethargy, sleepiness and lack of concentration during the day. Unilateral tonsil hypertrophy that is presumed to be neoplastic (tumour tonsillectomy) Chronic or recurrent tonsillitis, Cor-pulmonale 6/29/2022 44
- 46. Mgmt cnt… Contraindications Bleeding disorders Anemia Acute infection 6/29/2022 46
- 47. COMPLICATION 1. Chronic tonsillitis – incomplete resolution of acute tonsillitis 2. Peritonsillar abscess 3. Parapharyngeal abscess 4. Acute otitis media – recurrent attacks 5. Cervical abscess due to suppuration of jugulodigastric nodes 6. Rheumatic fever – group A B-hemolytic streptococci 7. Subacute bacterial endocarditis (patients with valvular heart disease) – streptococcus viridans. 8. Tonsilloliths (stones), tonsillar cysts, sleep apnoea 6/29/2022 47
- 48. Post-operative Complications Haemorrhage - the most common complication - intraoperative/primary (occurring within the first 24hrs) - secondary (occurring between 24hrs and 10 days) Pain (sore throat, otalgia) Dehydration (children - do not eat because of pain) Fever (not common, usually related to local infection Postoperative airway obstruction (uvular oedema, haematoma, aspirated material) 6/29/2022 48
- 49. Local trauma to oral tissues Temporomandibular joint dislocation Nasopharyngeal stenosis Death - uncommon - bleeding - or anaesthetic complications 6/29/2022 49
- 50. 6/29/2022 50
- 51. NURSING MANAGEMENT NANDA nursing diagnosis for TONSILLECTOMY 1. Pain related to inflammatory process/surgical operation. 2. Fluid volume deficit related to decreased fluid intake secondary to pain on swallowing. 3. Imbalanced nutrition less than body requirement related to reduced input secondary to pain on swallowing. 4. Hyperthermia related to related to acute infection by micro-organism. 6/29/2022 51
- 52. Diagnosis cnt… 5. Risk of ineffective airway clearance. 6. Impaired verbal communication. 7. Disturbed sleep pattern related to the pain in the tonsil area. 8. Risk for infection related to the factors of surgery. 9. Risk to the ineffectiveness of therapeutic management related to inadequate knowledge about the complication, pain, positioning and management activities. 6/29/2022 52
- 53. Implementation 1. Pain management Assess the level of pain and change in facial grimace. Monitor vital signs. Provide comfort measures e.g. changes in position, music, and relaxation. If prescribed analgesics, analgesics are routinely set during the first 24 hours, not waiting for patient to ask for it. 6/29/2022 53
- 54. Apply ice collar PRN to control pain and postoperative bleeding. To minimize nausea and vomiting, teach the patient to spit out secretions as much as possible. Provide lozengs to reduce sore throat 6/29/2022 54
- 55. 2. Promoting fluid intake Assess patient for effective swallowing. Collaborate with surgery and anesthesiology staff regarding need for administration of steroids to control swelling of uvula, as needed. Measure and record intake and output hourly. Assess skin turgor and moisture of mucous membranes. Administer IV fluids via infusion pump as ordered. Monitor IV site hourly. 6/29/2022 55
- 56. Once patient is conscious and reflex have returned, offer ice chips or lukewarm fluids. Do not offer straw, as this may precipitate bleeding. To minimize nausea and vomiting, teach the patient to spit out secretions as much as possible. Discourage excessive coughing, nose blowing or clearing of throat. Administer anti-emetics as prescribed to prevent vomiting. 6/29/2022 56
- 57. 3. Maintaining airway clearance. Assess for signs and symptoms of inadequate oxygenation. Place in the prone or side-lying position. Have a suction equipment available at the bedside. Teach and demonstrate breathing exercises. 6/29/2022 57
- 58. Observe for patent airway and possible laryngospasm due to swelling of uvula, palate, nasopharynx, retropharyngeal space, tongue and nose. Report any airway obstruction or laryngospasm to anesthesiology immediately; have oxygen and ambu bag available. Apply cool, humidified air per order, to minimize swelling, promote comfort and maintain oxygenation status. 6/29/2022 58
- 59. 4. Enhancing Knowledge Assess parents’ knowledge of the condition and management. Allow time for teaching, use a variety of methods (written instructions, pictures, verbal instruction), encourage questions and reassure about condition. Instruct to refrain from performing strenuous physical activity following surgery and may return to work/school once comfortable. 6/29/2022 59
- 60. Provide information about the surgery as needed. Teach that an important risk after a tonsillectomy, discourage excessive coughing and clearing the throat. Instruct parents to encourage to drink clear liquids during the first day, then shift to soft foods as per physician’s preference. Teach visitors how to evaluate for dehydration. Provide medication teaching as needed. 6/29/2022 60
- 61. 5. Reducing infection Monitor temp. every 4 hourly, the state of injury when performing maintenance. Give an antibiotics is prescribed, give at least two liters of fluid every day while implementing antibiotic therapy. Give antipyretics are prescribed if there is fever. 6/29/2022 61
- 62. Assess and observe surgical site for odor, irritation, inflammation, pus. Assess vital signs. Assess laboratory value WBC/fever, chills, blood culture. 6/29/2022 62
- 63. 6. Promoting communication Assess patient ability to understand the spoken word and expression. Provide call light. Paper pencil. Keep patient near the nursing station. Provide rest to the larynx or vocal cord to minimize pain and bleeding. 6/29/2022 63
- 64. Prevention Wash your hands often, especially before touching your nose or mouth. Avoid sharing food, drink, or utensils with someone who is sick. Replace toothbrush regularly. Gargle with warm salt water. Suck on lozenges with benzocaine or other medications to numb throat. Get lots of rest 6/29/2022 64
- 65. References 1. Mandal G.N (2016) “A Textbook of Medical Surgical Nursing”. 5th editionKathmandu.Makalu Publication House.2078/03/11 at 4:30 pm 2. Brunner and Suddarth, “Text Book of Medical and Surgical Nursing”, 12th edition, Wolter Kluwer India Private Limited 3. https://www.healthline.com/health/tonsillitis 4. https://www.slideshare.net/drangelosmith/tonsilli tis-38166423 6/29/2022 65
- 66. References cnt… 5.https://www.slideshare.net/vandanavalluri/tons illitis-48105665 6. https://www.mayoclinic.org/diseases- conditions/tonsillitis/symptoms-causes/syc- 20378479 7. Pubmed…current articles 2013 8. Current diagnosis & treatment in otolaryngology. 6/29/2022 66
- 67. 6/29/2022 67
- 68. 6/29/2022 68