Septic Arthritis
•Download as PPTX, PDF•
0 likes•114 views

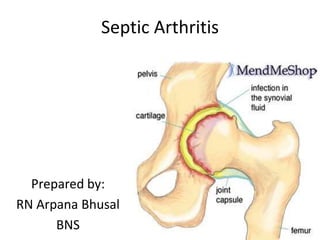
Septic Arthritis Inflammation of joint due to a bacterial or fungal infection. Its mainly occur due to pyogenic organism.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Septic Arthritis
Similar to Septic Arthritis (20)
More from government hospital
More from government hospital (20)
Recently uploaded
Recently uploaded (20)
Septic Arthritis
- 1. Septic Arthritis Prepared by: RN Arpana Bhusal BNS
- 3. Introduction Inflammation of joint due to a bacterial or fungal infection. Its mainly occur due to pyogenic organism. It presents as an acute painful arthritis, but it may present as subacute or chronic arthritis. It also named as infective arthritis, pyogenic arthritis or supporative arthritis
- 4. Causes Acute Septic Arthritis: Most common causative organism: Staph.aureus Other organisms are streptococcus, Pneumococcus and Gonoccus Chronic Septic arthritis: Mycobacterium Tuberculosis, Candida albucans Less common
- 5. Routes of Infection Hematogenous: It is most commonest route and may be a primary focus ofinfection in the form of pyoderma, throat infection and septicemia. Secondary to near by Oteomyelitis: Particularly common route in joints with intra-articular metaphysis. E.g hip,shoulder. Penetrating wounds: The knee, being a superficial joint, I soften affected via this route. Iatrogenic: It may occur following intra-articular steroid injection in different arthritis and during femoral artery punctures for blood collection. Umbilical cord sepsis: Infection can travel to joints
- 6. Risk Factors Artificial joint implants Bacterial infection somewhere else in your body Chronic illness or disease (such as diabetes, rheumatoid arthritis, and sickle cell disease) Intravenous (IV) or injection drug use Medications that suppress your immune system Recent joint injury Recent joint arthroscopy or other surgery Seen at any age Children younger than 3 years( Hip)
- 7. Pathogenesis ) Any one of the etiology enter to the body through various route, it reaches to the joint. Begin an inflammatory response in the synovium which resulting in the exudation of fluid within the joint. Joint cartilage is destroyed by inflammatory grannulation tissue and lysosomal enzymes in the joint exudate. Destruction of the joints and loss of joint movement(ankylosis).
- 8. Clinical Features ) In a typical acute form: -Severe throbing pain -Swelling -Redness of the affected joint associated with high grade fever and malaise. -Unable to use affected limb In subacute phase: -- Not allowing to touch the affected joint -Low grade fever
- 9. Clinical Features ) Not moving the affected limb properly due to pain on movement Joint Swelling just one joint Psuedoparalysis Joint tenderness
- 10. Diagnosis mainly clinical examination Aspiration of joint fluid for cell count, examination of crystal under the microscope, gram stain & culture. Blood Culture Blood: Neutrophil leukocytosis, ESR increased
- 11. Diagnosis X-Ray of affected joint: shows joint space soft tissue
- 12. Treatment Antibiotic: - In joint infections, parenteral antibiotics - at least 2 weeks. -Infection with either methicillin-resistant S aureus or methicillin- susceptible S aureus - at least 4 full weeks IV antibiotic therapy. -Orally administered antimicrobial agents are almost never indicated in the treatment of S aureus infections. -Gram-negative native joint infections with a pathogen i.e sensitive to quinolones can be treated with oral ciprofloxacin for the final 1-2 weeks of treatment. -2-week course of intravenous antibiotics is sufficient to treat gonococcal arthritis. -Drugs Used: Ceftriazone, Cifrofloxacin, Cefixime, Oxacillin, Vancomycin
- 13. Contd………. Joint immobilization and physical therapy -Resting, keeping the joint still, raising the joint and using cold compresses may help relieve pain. -Immobilization of the joints to control the pain. -Exercising the affected joint helps the recovery process. Arthrocentesis -If synovial fluid builds up quickly due to the infection, a needle may be inserted into the joint often to aspirate the fluid. Severe cases may need surgery to drain the infected joint fluid. Physical Therapy -Usually, immobilization of the infected joint to control pain is not necessary after the first few days. -If the patient's condition responds adequately after 5 days of treatment, begin gentle mobilization of the infected joint.
- 14. Contd….. - Most patients require aggressive physical therapy to allow maximum postinfection functioning of the joint. -The joint should bear no weight until the clinical signs and symptoms of synovitis have resolved. Synovial Fluid Drainage: -In general, use a needle aspirate initially,repeating joint taps frequently enough to prevent significant reaccumulation of fluid. -Aspirating the joint 2-3 times a day may be necessary during the first few days. -If frequent drainage is necessary, surgical drainage becomes more attractive. - Gonococcal-infected joints rarely require surgical drainage.
- 15. Contd….. Indication for Surgical drainage: -The appropriate choice of antibiotic and vigorous percutaneous drainage fails to clear the infection after 5-7 days. -The infected joints are difficult to aspirate (eg, hip). -Adjacent soft tissue is infected. Prognosis -Recovery is good with prompt antibiotic treatment. If treatment is delayed, permanent joint damage may result. Complications Deformity & stiffness Pathological dislocation Osteoarthritis
- 16. THANK YOU