10. INTRODUCTION
• Spinal cord injury (SCI) is a major
health problem. Before world war II ,
the life expectancy for a person with
a spinal cord injury ranged from
months to 10 years from the onset of
injury. Today , with improved
treatment strategies , even a very
young patient with SCI can anticipate
a long life.
11. Definition
•A spinal cord injury (SCI)
refers to any injury to
the spinal cord that is
caused by trauma
instead of disease.
12. DEFINITION 2
•Spinal cord injury (SCI) is
damage to the spinal cord
that results in a loss of
function such as mobility
or feeling.
13. Incidence
• Spinal cord injury occurs
almost four times more often
in males than females. Young
people aged 16 to 30 suffer
more than half of the new SCI
each year.
14. Risk factors
• Age
• Gender
• Alcohol
• Drug use
The vertebrae most frequently
involved in SCI are the 5th, 6th,7th
cervical (Neck), the 12th thoracic, and
the 1st lumbar vertebrae.
18. HYPERFLEXION
• WHEN A PERSON STRIKES THE HEAD
AGAINST THE STEERING WHEEL OR
WINDSHIELD, THE SPINE IS FORCED
INTO ACUTE HYPERFLEXION.
• CERVICAL SPINE C5-6 IS MOST
COMMONLY AFEECTED.
22. COMPRESSION INJURIES
• Compression injuries are often
caused by falls or jumps in which
the person lands directly on the
head, sacrum or feet. The lumbar
and lower thoracic vertebrae are
the most commonly injured
regions.
23.
24. LEVEL OF INJURY
• SKELETAL LEVEL OF INJURY
Injury is to the vertebral level
where there is the most
damage to vertebral bones
and ligaments.
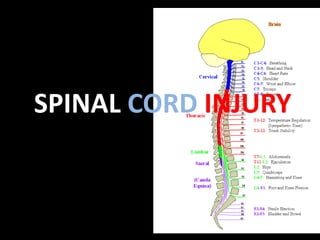
25. Neurological Level of injury
The level of injury may be cervical,
thoracic or lumbar. If cervical cord is
involved, paralysis of all four
extremities occurs, resulting in
tetraplegia. If the thoracic or
lumbar cord is damaged, it may lead
to paraplegia.
26. Degree of injury
• The degree of spinal cord
involvement may be either complete
cord involvement or incomplete
(partial).
28. Incomplete cord involvement
• It results in a mixed loss of
voluntary motor activity and
sensation and leaves some tracts
intact. Six syndromes are
associated with incomplete
lesion:
30. Central cord syndrome
• Damage to the central spinal cord
which occurs most commonly in the
cervical cord region. Motor weakness
and sensory loss are present in both
the upper and lower extremities, but
the upper extremities are affected
more than lower ones.
31.
32. Anterior cord syndrome
• It is caused by damage to the anterior
spinal artery . This results in
compromised blood flow to the anterior
spinal cord due to compression of the
anterior portion of the spinal cord.
Manifestations include motor paralysis
and loss of pain and temperature
sensation below the level of injury.
33.
34. Brown-Sequard syndrome
• It is the result of damage to one half of
the spinal cord. This syndrome is
characterized by a loss of motor function
and position and vibratory sense, as well
as vasomotor paralysis on the same side
(ipsilateral) as the lesion. The opposite
(contralateral) side has a loss of pain and
temperature sensation below the level of
lesion.
35.
36. Posterior cord syndrome
• It results from compression or
damage to posterior spinal artery.
Motor function remains intact
but the client experiences a loss
of vibratory sense, discriminative
touch and proprioception.
37. Cauda equina syndrome and Conus
medullaris syndrome
•It results from damage to
the very lowest portion of
the spinal cord (conus) and
the lumbar and sacral
nerve roots (cauda equina).
38. Other SCI types
• CONCUSSION: causes a temporary loss
of functions lasting for 24 to 48 hours.
• CONTUSION: it is the bruising of the
cord that includes bleeding into the
cord with subsequent edema and
possible necrosis.
• TRANSECTION :is the severing of the
cord that can be complete or
incomplete.
40. SPINAL CORD INJURY
SECONDARY INJURIES
PRIMARY INJURIES
DUE TO INITIAL
INSULT OR
TRAUMA
SWELLING AND
DEGENERATION OF NERVE
FIBRE
ISCHEMIA
HYPOXIA
EDEMA
DESTRUCTION OF MYELIN AND
AXON
41. CLINICAL MANIFESTATIONS
• Total sensory and motor paralysis
• Loss of bladder and bowel control
• Loss of sweating
• Decreased blood pressure due to loss of
peripheral vascular resistance
• Paraplegia (paralysis of lower body)
• Quadriplegia (paralysis of all four extremities)
42. • Acute pain in back and neck
• Respiratory dysfunction
• Pressure ulcers due to lack of movement
43. Cervical injury manifestations
• Involvement above C4 causes
respiratory difficulty and
tetraplegia.
• Injury at C5 through C8 may have
decreased respiratory reserve.
• Injury at C2 to C3 is usually fatal
44. Thoracic level injuries
• Loss of movement of the chest, trunk, bowel
bladder and legs depending on the level of
injury.
• Paraplegia
• Autonomic dysreflexia ( above T6and in cervical
lesion)
• Distended bladder, impacted rectum and may
cause reactions such as sweating, bradycardia,
hypertension and goose flesh.
45. Lumbar and sacral level injuries
• Loss of movement and sensation of
the lower extremities
• Neurogenic bladder
• Injury above S2 in males may have
erection but unable to ejaculate.
•
46. Diagnostic studies
• History of neurological trauma
• Neurological Examination
• X-ray of spine
• C.T
• M.R.I
• Myelography
• Lumbar puncture
49. Other therapy
• Respiratory therapy- oxygen is
administered to maintain a high
arterial PO2 because hypoxemia can
worse neurologic condition.
• Skeletal fracture reduction and
traction with use of halo device.
• Cervical collar to reduce dislocations.
53. complications
• Spinal and neurogenic shock
• Deep vein thrombosis
• Pressure ulcers
• Orthostatic hypotension
• Autonomic dysreflexia ( characterized by
headache, profuse seating, nasal
congestion ,goose bumps, bradycardia
and hypertension)
54. Nursing diagnosis
• Impaired gas exchange related to
intercostal muscle paralysis as
evidenced by decreased PaO2.
• Impaired skin integrity related to
immobility as evidenced by
reddened skin
55. Cont…
• Impaired urinary elimination related to
spinal injury as evidenced by urinary
retention.
• Ineffective coping related to loss of
control over bodily functions and altered
life style secondary to paralysis as
evidenced by verbalization of inability to
cope.
Editor's Notes
It is massive uncompensated cardiovascular reaction mediated by SNS.
Type of bladder dysfunction related to abnormal or absent bladder innervation.