Pelvic inflammatory disease
•Download as PPTX, PDF•
4 likes•599 views

pelvic inflammatory disease is the infectious disease in the female upper genital organ and its causes discomfort to the patient and knowledge of this ppt can help the patients and nurses to know the disease process well and can apply this knowledge into their clinical practices

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Pelvic inflammatory disease
Similar to Pelvic inflammatory disease (20)
More from Pallavi Lokhande
More from Pallavi Lokhande (20)
Recently uploaded
Recently uploaded (20)
Pelvic inflammatory disease
- 1. PELVIC INFLAMMATORY DISEASE DEPARTMENT OF MEDICAL SURGICAL NURSING
- 2. LEARNING OBJECTIVE At the end of this lecture, students should be able to: define PID enlist the causes of PID discuss the pathophysiology of PID list down the clinical manifestation and investigation of PID discuss the complication and treatment of PID
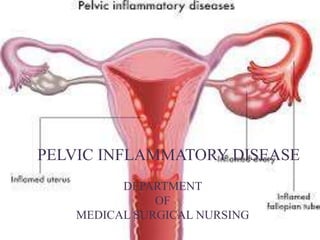
- 3. DEFINITION • Pelvic inflammatory disease is a spectrum of infection and inflammation of the upper genital tract organs • typically involving the Endometrium, fallopian tubes, ovaries, pelvic peritoneum and surrounding structures.
- 6. • Many types of bacteria can cause PID, but gonorrhea or chlamydia infections are the most common. • unprotected sex. • Child birth, miscarriage, abortion • Being a sexually active woman younger than 25 years old • Having multiple sexual partners • Being in a sexual relationship with a person who has more than one sex partner • Douching regularly, which upsets the balance of good versus harmful bacteria in the vagina and might mask symptoms • Having a history of pelvic inflammatory disease or a sexually transmitted infection
- 7. PATHOPHYSIOLOGY • The involvement of the tubes is almost bilateral • The pathogical process is initiated primarily in the endosalpinx. • There is gross destruction of the epithelial cells, cilia and microvilli.
- 8. • In severe infection, it invades all the layers of the tube and produces acute inflammatory reaction, becomes edematous and hyperemic. • Closure of both the ostia results - the exudates inside the tube.
- 9. • The exudates pours through the abdominal ostum to produce pelvic peritonitis • and pelvic abscess or may affects the ovary producing ovarian abscess. • Thus a tube ovarian abscess.
- 10. CLINICAL FEATURES SYMPTOMS • Bilateral lower abdominal and pelvic pain • Fever, lassitude(mental and physical wearing, lack of energy), headache • Irregular and excessive vaginal bleeding • Abnormal vaginal discharge
- 11. • Nausea and vomiting. • Dyspareunia - difficulty or painful intercourse • Pain and discomfort in the right hypochondrium.
- 12. CLINICAL FEATURES • SIGNS • Temperature – 38.30 c • Tenderness on both quadrants of lower abdomen • Liver enlarged and tender. • Vaginal examination reveals
- 13. • Abnormal vaginal discharge – purulent. • Congested external urethral meatus • Bimanual examination reveals - bilateral tenderness on fornix palpation - thickening or a definite mass felt through the fornices.
- 14. INVESTIGATIONS IDENTIFICATION OF ORGANISMS • Discharge from the urethra or Bartholin’s gland • Cervical canal • Collected pus from the fallopian tubes during laparoscopy or laparotomy
- 15. BLOOD • Leukocyte count -10,000 per cu mm and • an elevated ESR value of more than 15mm per hour. • Serological test
- 16. LAPAROSCOPIC FINDINGS AND SEVERITY OF PID • Hyperaemia and edema of the tubes • Purulent exudates from the fimbrial ends SONOGRAPHY • Dilated and fluid- filled tubes, • fluid in the pouch of Douglas or • adnexal mass are suggestive of PID
- 17. COMPLICATIONS IMMEDIATE • Pelvic peritonitis or generalized peritonitis • Septicaemia – producing arthritis or myocarditis LATE • Dyspareunia • Infertility • Chronic pelvic inflammation
- 18. TREATMENT Essential Steps In The Prevention • Community based approach • Prevention of sexually transmitted disease • Liberal use of contraceptives • Routines screening of high-risk population
- 19. The Principles of Therapy • To control the infection energetically • To prevent infertility and late sequelae. • To prevent reinfection • Out Patient Therapy • Antibiotic therapy
- 20. IN- PATIENT THERAPY • Hospitalization for antibiotic therapy • Bed rest • oral feeding is restricted • Dehydration and acidosis - to be corrected
- 21. In patient antibiotic therapy • Cefoxitin 2mg IV 4 times a day for 2-4 days • Gentamycin 2 mg / kg IV ( loading dose ) following by 1.5 mg / kg IV (maintenance dose) every 8 hours. • Metronidazole 500 mg IV every 8 hours.
- 22. Indication Of Surgery • Generalized peritonitis • Pelvic abscess • Tubo- ovarian abscess
- 23. Summary So far we have discussed about definition, causes, pathophysiology, clinical manifestations, investigations, complications and managements of PID.
- 24. Bibliography • Lewis et al, Medical Surgical Nursing, Mosby Elsevier,7th edition. • Joyce.M.Black et al, Medical Surgical Nursing, Saunders publication. • Brunner and Siddhartha, Medical Surgical Nursing, Lippincott Williams and Wilkins.
- 25. Thank You