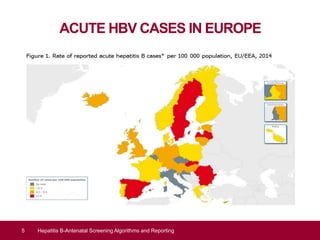
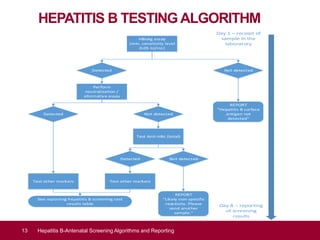
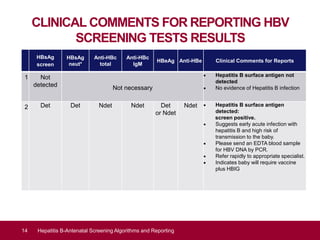
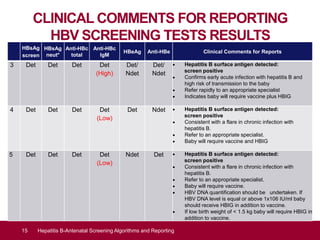
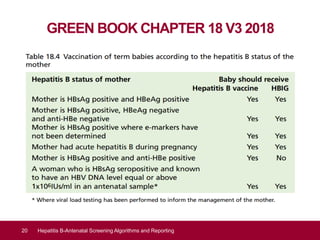
This document discusses hepatitis B screening algorithms and reporting for pregnant women in the UK. It provides background on the national screening program and standards for viral hepatitis B screening during pregnancy. The goals of antenatal hepatitis B screening are early detection of infection to enable treatment for the mother and reduce mother-to-child transmission risk by offering newborn vaccination and prophylaxis. The document reviews epidemiology data on acute hepatitis B cases in Europe and England and outlines the clinical outcome and diagnosis of hepatitis B infection through various serological markers. It presents the hepatitis B testing algorithm and provides clinical comments for reporting screening test results.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
