
Recommended
More Related Content
What's hot
What's hot (20)
Similar to CPB(CARDIO PULMONARY BYPASS)
Similar to CPB(CARDIO PULMONARY BYPASS) (20)
More from DR NIKUNJ SHEKHADA
More from DR NIKUNJ SHEKHADA (20)
Recently uploaded
Recently uploaded (20)
CPB(CARDIO PULMONARY BYPASS)
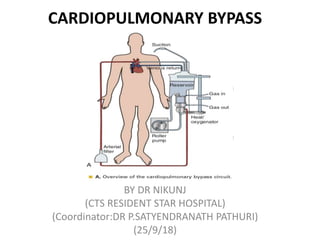
- 1. CARDIOPULMONARY BYPASS BY DR NIKUNJ (CTS RESIDENT STAR HOSPITAL) (Coordinator:DR P.SATYENDRANATH PATHURI) (25/9/18)
- 2. • Cardiopulmonary bypass (CPB) is one of the most important biomedical inventions in the history of health care
- 3. HISTORY • 1812: Le Gallois showed that extracorporeal circulation is Possible, part of the body might be preserved by some sort of external perfusion device. Tissues and organs of apparently dead animals could be brought back temporarily to an apparent living state by restoring the flow of blood to them. • 1858: Brown-Sequard arterialized desaturated blood. He used syringes for perfusion and put oxygen into the dark venous blood by beating the blood vigorously. An interesting observation he made was the temporary disappearance of the rigor mortis of muscles of guillotined animals when they were perfused with their own blood, it was evident that supplying an adequate amount of oxygen to the blood is essential for successful perfusion. • 1882: first “bubble”-oxygenator by von Schroeder Bubbling method was based on the supposition that bubbles of a gas, such as air or oxygen passing through blood, would become surrounded by a thin layer of the blood that in turn would absorb oxygen, give off carbon dioxide, and then burst and leave the blood free of gas. Drawback: foaming of the blood and gas embolism
- 4. HISTORY • 1885: first “film”-type oxygenator Filming Method It is best technique for oxygenating the blood, the one that would form the basis of techniques currently in use. Von Frey and Gruber achieved this objective by dispersing the blood as a thin film inside a rotating slanted cylinder filled with oxygen. • 1890: Jacob j described an device with a bubble oxygenator & bladder pump in order to provide pulsatile flow (oxygenating the blood with a mechanical device altogether by accomplishing this objective through the use of the animal's own lungs) • 1916: discovery of heparin by McLean significant step in evolution of heart-lung-machine • 1928: Dale & Schuster described the prototype pumping mechanism (valved pump) • 1934: Debakey modified the twin roller pump
- 5. • 1929: BRUKHONENKO • He perfused Guillotined head of a dog. • This preparation relied on gas exchange from a second donor dog's lungs. • Diaphragm-like pumps pumped blood into the recipient dog's carotid arteries. • Dog heads perfused in this manner remained functional for a few hours.
- 6. BIRTH OF AN IDEA AND THE DEVELOPMENT OF CARDIOPULMONARY BYPASS • a patient in distress • It was mid afternoon on October 3, 1930 and a patient at the Massachusetts General Hospital in Boston. • For 2 weeks her convalescence from an uncomplicated cholecystectomy had been uneventful. • she suddenly developed discomfort in her right chest, and immediately the discomfort gave way to sharp pain. • Dr. Edward Churchill, who saw her at once in consultation, found her frightened, pale, cyanotic, cold, and moist. • John H. Gibbon, Jr. was assigned the task of watching the patient and monitoring her vital signs • He believed that the diagnosis of massive pulmonary embolism. • she was moved to the operating room where pulmonary embolectomy done. • “Idea naturally occurred to him that if it we continuously remove some of the blue blood from the patient's swollen veins, put oxygen into that blood and allow carbon dioxide to escape from it, and then inject continuously red blood back into the patient's arteries, we might have saved her life. We would have bypassed the obstructing embolus and performed part of the work of the patient's heart and lungs outside the body”
- 7. • Gibbon planned to build an apparatus with the oxygenating capacity, which permit safe total CPB in humans. • Gibbon later estimated that if this objective were achieved using the rotating drum technique. • Dr.Gibbons, inventor of the cardio-pulmonary bypass machine. • • 1935 –He maintained a cat’s circulation on CPB while closing the pulmonary artery
- 8. • University of Minnesota • Hospital operating room on September 2, 1952 near the end of the first successful open heart operation in medical history. • Dr. F. John Lewis closed an atrial septal defect under direct visualization using inflow stasis and moderate total body hypothermia (26°C). • In a 5-year-old girl who remains alive and well today. • Postoperative heart catheterization confirmed a complete closure.
- 9. • 1953:JohnGibbon • Cecelia Bavolek First patient to undergo open heart surgery using CPB to repair an atrial septal defect. • Just as Gibbon was ready to close the defect, the oxygen saturation of the blood began to rapidly fall, and clots began to form on the oxygenator screens because of inadequate heparinization.
- 10. AZYGOUS FLOW PRINCIPLE • Morley cohen during some canine experiments in which the cavae were temporarily occluded to test tolerance limits of the brain and heart to ischemia. • It was discovered that if the azygos vein was not clamped the resulting very small cardiac output (8 to 14 mL/kg body weight/min) was sufficient to sustain the vital organs safely in animals for a minimum of 30 minutes at normothermia.
- 11. Cardiopulmonary Bypass • Controlled Cross-circulation • 1954. LILLEHEI 1st surgical closure of VSD under controlled cross- circulation. • Based on placental function & azygous flow principle. • Used in 45 patients between 1954 to 1955. • VSD ,TOF .
- 12. • March 26, 1954: • University of Minnesota • Medical Center, during the • first controlled cross- circulation operation. • VSD was successfully visualized by ventricular cardiotomy and closed in a 12- month-old infant. The lightly anesthetized donor • ( patient's father) with the groin cannulations serving as the extracorporeal oxygenator. The VSD was closed by direct suture during a bypass time of 19 minutes.
- 13. • 1955: Mayo Clinic-Gibbon heart lung machine (screen oxygenator + rollar pump) . This model was used in first series of open heart operations performed by Dr. John Kirklin and associates • at the Mayo Clinic
- 14. More than 30 years of Innovation, Research, and Hard Work
- 15. • 1951. Dodrill. Mitral valve surgery under left heart bypass • 1952. Dodrill. Relief of PS under right heart bypass • 1952. Lewis. ASD closure under surface cooling • 1953. Gibbon. ASD closure by heart-lung machine • 1954. Lillihei. VSD closure under controlled cross- circulation • 1954. Kirklin. Establishment of CPB with oxygenator in cardiac surgery
- 16. FUNCTIONS OF CPB • Diversion of blood from heart • Oxygenation, elimination of CO2 • Systemic cooling and rewarming • Circulation of blood. • Non physiological hypothermic hemodiluted non pulsatile circulation.
- 17. PRINCIPLES OF CPB • HYPOTHERMIA • HEMODILUTION • ULTRAFILTRATION • ANTICOAGULATION & NEUTRALIZATION
- 18. HYPOTHERMIA • Feasibility and applicability of hypothermia for heart surgery was first suggested by Bigelow and colleagues in (1950) • Rationale – provide organ protection and safety margin during CPB • ↓ metabolic rate and o2 consumption. • Preserve high energy po2 store and ↓ excitatory NT release. • Lower pump flows suffice- ↓return, improve visibility, less blood trauma. • Better myocardial protection. • Safety margin in equipment failure.
- 19. EFFECT OF HYPOTHERMIA ON MYOCARDIUM • Basal myocardial O2 requirement is 10 ml/100g/min • In the asystolic state this goes down to 0.1 ml/100g/min • For every 10 degree drop in temperature there is an additional 50% decrease in O2 requirements. • However there is a potential for myocardial damage below 10 degrees due to damage to the membrane enzymes responsible for cellular integrity. • Therefore target myocardial temperatures are usually 10-15 degrees
- 20. EFFECT OF HYPOTHERMIA Heart • ↓HR • ↑Contractility ↑dysarythmia Coronary b f preserved Lungs • progressive↓ in ventilation • Gas exchange unchanged • Kidney • ↓renal b f ↓concentrating ability Glycosuria. Liver • ↓ metabolic & excretory function • Marked hyperglycemia blood vessels: vasoconstriction-skeletal muscles and extremities Blood :↑ blood viscosity • RBC- aggregation Portal platelet sequestration Complement activation, catecholamine release Bradykinnin release.
- 21. Brain- • With a linear decrease in CBF, CMRO2 decreases exponentially. • At normothermia CBF/CMRO2 of 20:1 changes to 75:1 at deep hypothermia.
- 23. ACID BASE MANAGEMENT IN HYPOTHERMIA • ALPHA STAT • Alpha = unprotonated histidine imidazole group/[H+] • total CO2 content kept constant • PH & PCO2 is allowed to vary with temperature • PH STAT • pH kept constant at all temperatures
- 24. ALPHA STAT Vs PH STAT • ALPHA STAT • Less but adequate cerebral flow • Better cerebral recovery • Cerebral autoregulation • preserved • Less arrhythmias • Better in adults PH STAT • Increased CBF • Global cerebral cooling • Better flow to deep brain structures • ↑ risk microemboli, cerebral edema, ↑icp, redistribution away from marginally perfused area • Better in children
- 25. HEMODILUTION • CPB • ↓ flow rate & hypothermia → ↑viscosity • ↑ vascular resistance • Hemodilution • ↓ Hct → shear rate increasebridges disintegrate ↓viscosity improve microperfusion.
- 26. HEMODILUTION Advantages ↓ CPB complications • Good tissue perfusion • Good oxygen delivery Disadvantages • ↓plasma colloid oncotic pressure ↓plasma protein conc( PK & PD of drugs) ↓coagulation factor/ platelet conc ↓immunoglobulin conc. • Extreme hemodilution cause inadequate O2 delivery. • At 25%- myocardial O2 extraction is complete. • < 15%- maldistribution of coronary flow from sub endocardium. • Target HCT- 20-25% • Prime – crystalloid + colloid
- 27. FLOW RATES, PERFUSION PRESSUR AND AUTOREGULATION • Flow is generally kept in the range of 2.2 to 2.5 liter/min/ m2 to provide a margin of safety during CPB, because systemic blood flow distribution and O2 consumption remain normal at this level. • At normothermia, a target mean blood pressure of 50 to 70 mm Hg is used. (As a rule of thumb in adults, the mean pressure chosen should be equal to the patient’s age.) • Autoregulation of CBF is also related to changes in perfusion pressure. At normothermia, a mean pressure of 50 mm Hg is the threshold at which the brain autoregulates flow, but with hypothermia (26°C), the threshold drops to 30 mm Hg . At deep hypothermia (<20°C), there is a loss of pressure- flow autoregulation, as severe temperature reductions impair cerebral vascular relaxation and changes in cerebral perfusion pressure alone result in corresponding proportional changes in CBF.
- 28. • Flow Rates In Hypothermia: • 32 c: 2.1 to 2.2 lit / min /m2. • 30 c: 1.8 to 1.9 lit / min /m2. • 25 c: 1.6 lit / min /m2. • 20 c: 1.4 to 1.5 lit / min /m2. • 15 c: 1 to 1.1 lit / min /m2.
- 29. • The two commonly used types of pumps for CPB involve either roller or centrifugal fluid propulsion. • • Roller • noninterrupted contact of the rollers with the tubing in the track results in the nonpulsatile nature of the flow . • Flow is calculated from the RPM of the roller pump knowing the diameter of the tubing and thus precisely the volume displaced. • A low compression will result in inadequate flow, whereas excessive compression may aggravate hemolysis and tubing wear. Other complications associated with the use of the roller pump include (1) cavitation caused by excess pressure and (2) spallation (the release of particles from the inner surface).
- 30. • centrifugal • A rotating impeller spins at 2000 to 5000 revolutions per minute on a small bearing, or the blades are magnetically suspended. This creates a vortex that draws blood into the pumphead and thrusts it to the oxygenator. • The advantages of this device include its relatively small priming volume • with a roller pump, venous drainage to the reservoir from the patient is dependent on gravity drainage, centrifugal pumps are not constrained by this action. • these devices are susceptible to air locks, thus requiring vigilance by the perfusionist • power outage with a centrifugal pump can be a disaster
- 31. ULTRAFILTRATION • Reverses the `hemodilution` during CPB initiation and Optimises perfusate Hct • Raises colloid osmotic pressure • Decreases post CPB edema and weight gain • Improved tissue perfusion and oxygenation • Removes the vasoactive substances eg. C3a, C5a, TNF-α, IL-1b, IL-6, IL-8 • Improves hemostasis - increasing relative conc. of clotting factors
- 32. PRINCIPLES OF ULTRAFILTRATION • Filtration rate – • Directly proportional to transmembrane pressure gradient & inversely proportional to Hct. • Concentration of all molecules smaller than smallest pores equal on both sides of the membrane. • Conc. of molecules larger than the smallest pores, but smaller than the largest pores is dependent on the sieving coefficient of that molecule. • No fluid is given to replace that removed- creates negative balance
- 33. MONITORING PERFUSION ADEQUECY • Systemic measurements that indicates adequecy of perfusion are • 1) Svo2 2) Ph 3) lactate concentration • Venous Saturation • High Svo2 does not mean adequate perfusion • Low Svo2 indicates inadequate tissue perfusion. • Relation b/w perfusion and O2 consumption • Oxygen consumption plateauing • Vo2 optimization. • Disadvantage: • Vo2 is calculated for awake or anesthetized prebypass volume. • During CPB with hypothermia baseline Vo2 would yield excess perfusion during CPB.
- 34. THANK YOU