2. SPECIFIC LEARNING OBJECTIVES
• Indications, Contraindications and Side Effects of LMA use.
• The steps necessary to prepare for LMA placement.
• The methods of LMA placement.
• Problems associated with LMA placement.
3. INTRODUCTION
• LMA is a minimally invasive device designed for the
management of the airway in unconscious patients.
• It has been used in more than 200 million patients
worldwide with no reported fatalities.
• Introduced into American society of Anaesthesiologists
{ASA} difficult airway management algorithm in
1995.
4. • Features of an ideal supraglottic airway device
• It should efficiently seal the upper airway during spontaneous
and positive pressure ventilation
• Should have low resistance to respiratory gas flow
• It should protect subglottic airway from upper airway
secretions and gastric contents
• Should have low incidence of airway morbidity and adverse
effects
• The shape, material ,cuff volume, cuff position should be such
that it is easily accepted by the oropharynx.
5. The LMA was invented by Dr. Archie Brain at the
London Hospital, Whitechapel in 1988
The LMA consists of two parts:
The mask
The tube
The LMA has proven to be very effective in the
management of airway crisis
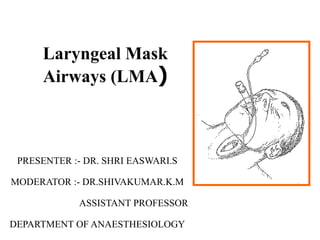
6. The LMA design:
• Provides an “oval seal around the
laryngeal inlet” once the LMA is
inserted and the cuff inflated.
• Once inserted, it lies at the
crossroads of the digestive and
respiratory tracts.
7. Indications for the
use of the LMA
• Situations involving a difficult mask (BVM) fit.
• May be used as a back-up device where endotracheal
intubation is not successful.
8. USING THE LMA FAMILY
• SIZE SELECTION
• PRE USE INSPECTION
• MASK PREPARATION
• ANESTHETIC INDUCTION
• AWAKE PLACEMENT
• CUFF INFLATION AND ASSESSING POSITION
AND FUNCTION
• FIXATION
9. • INTRA OPERATIVE MANAGEMENT
• EMERGENCE FROM ANESTHESIA
• CARE AND CLEANING
• LIFE SPAN
• DEAD SPACE
• FLOW RESISTANCE AND WORK OF BREATHING
10. Size Selection
Verify that the size of the LMA is correct for the
patient
Recommended Size guidelines:
Size 1: under 5 kg
Size 1.5: 5 to 10 kg
Size 2: 10 to 20 kg
Size 2.5: 20 to 30 kg
Size 3: 30 kg to 40kg
Size 4: 40kg to 50kg
Size 5: >50kg
11. PRE USE INSPECTION
• Visually inspect the LMA cuff for tears or other abnormalities
• Inspect the tube to ensure that it is free of blockage, cuts or loose
particles and kinking of the spiral wires
• Deflate the cuff to ensure that it will maintain a vacuum
• Inflate the cuff to ensure that it does not leak
• The connector should fit tightly to the outer end of the airway
tube
12. Deflation and Inflation of the LMA
• Slowly deflate the cuff to form a smooth flat wedge
shape which will pass easily around the back of the
tongue and behind the epiglottis.
• During inflation the maximum air in cuff should
not exceed:
• Size 1: 4 ml
• Size 1.5: 7 ml
• Size 2: 10 ml
• Size 2.5: 14 ml
• Size 3: 20 ml
• Size 4: 30 ml
• Size 5: 40 ml
13. Mask Preparation
• Use a water soluble lubricant to lubricate the LMA
• Only lubricate the LMA just prior to insertion
• Lubricate the back of the mask thoroughly
• Important Notice:
• Avoid excessive amounts of lubricant
• on the anterior surface of the cuff or
• in the bowl of the mask.
• Inhalation of the lubricant following placement may result in
coughing or obstruction.
14. Positioning
of the Airway
• Extend the head and flex the neck
• Avoid LMA fold over:
• Assistant pulls the lower jaw
downwards.
• Visualize the posterior oral
airway.
• Ensure that the LMA is not
folding over in the oral cavity
as it is inserted.
15. ANAESTHETIC INDUCTION
• Requires sufficient general or topical anaesthesia to
obtund the airway reflexes
• Absence of motor response to a jaw thrust indicates
adequacy of anaesthesia for LMA insertion
• Greater depth required for LMA proseal than for LMA
classic
16. AWAKE PLACEMENT
• LMA can be inserted in awake patients following
topical anaesthesia of the upper airways or nerve
blocks
• Mask insertion should be co-ordinated with
swallowing [ partial inflation of the cuff may stimulate
bolus of food & may be helpful in insertion]
17. LMA INSERTION TECHNIQUES
• STANDARD TECHNIQUE
• 180 DEGREE TECHNIQUE
• PARTIAL INFLATION TECHNIQUE
• THUMB INSERTION TECHNIQUE
20. LMA Insertion Step 1
• Grasp the LMA by the tube,
holding it like a pen as near
as possible to the mask end.
• Place the tip of the LMA
against the inner surface of
the patient’s upper teeth
21. LMA Insertion Step 2
• Under direct vision:
• Press the mask tip upwards
against the hard palate to flatten
it out.
• Using the index finger, keep
pressing upwards as you advance
the mask into the pharynx to
ensure the tip remains flattened
and avoids the tongue.
22. LMA Insertion Step 3
• Keep the neck flexed and head
extended:
• Press the mask into the
posterior pharyngeal wall
using the index finger.
23. LMA Insertion Step 4
• Continue pushing with your
index finger.
• Guide the mask
downward into position.
24. LMA Insertion Step 5
• Grasp the tube firmly with the
other hand
• then withdraw your index
finger from the pharynx.
• Press gently downward with
your other hand to ensure the
mask is fully inserted.
25. LMA Insertion Step 6
• Inflate the mask with the
recommended volume of air.
• Do not over-inflate the LMA.
• Do not touch the LMA tube while it is
being inflated unless the position is
obviously unstable.
• Normally the mask should be allowed to
rise up slightly out of the hypopharynx as
it is inflated to find its correct position.
26. 180 DEGREE TECHNIQUE
• LMA inserted with laryngeal aperture pointing
cephalad & rotate it 180 degrees as it enters
hypopharynx
• Satisfactory as standard technique especially in
paediatric patients
• Draw back- bulky cuff in close proximity to
hypopharynx could dislocate arytenoid cartilage
27. PARTIAL INFLATION TECHNIQUE
• Cuff partially or fully inflated before insertion
• Incidence of sore throat is reduced
28. THUMB INSERTION TECHNIQUE
• Suitable in patients where access to head from behind is
difficult
• Similar to standard technique except that LMA is held
with thumb in the position instead of index finger
29. CUFF INFLATION & ASSESSING THE
POSITION
• Cuff should be inflated to pressure of approximately 60 cm of H2O over 3-
5 seconds without holding the tube
• This usually causes slight upward movement of the airway tube & oval
bulging at the front of the neck & no visible cuff in the oral cavity
• Cuff size is more important than the inflating volume in determining the
seal or leak pressure
• In positive pressure ventilation, leak pressure should be greater than 20 cm
H2O [30 cm H2O for LMA proseal]
• In spontaneous ventilation leak pressure should be greater than 20 cm H2O
30. Verify Placement of the LMA
• Connect the LMA to Bain’s circuit & ventilate
• Observe chest movements
• Normal breath sounds on auscultation
• Volume monitoring not showing a leak
31. Verify Placement of the LMA
• Carbon dioxide waveforms with positive pressure
ventilation
• Reservoir bag excursions in spontaneous ventilation
• Fiberscope or rigid endoscope can be inserted through
the LMA to confirm its position & rule out obstruction
• Oesophageal detector, x-ray or MRI can be used to
confirm its position
32. Securing the LMA
• Insert a bite-block or roll of gauze to prevent occlusion of
the tube should the patient bite down & to improve the
stability. [Not necessary for LMA proseal]
• Oropharyngeal airway if used with LMA may compress the
LMA cuff or tube as both are designed to be placed in
midline
• Tube should be secured with tape taking care that it doesn’t
become twisted or obstruct the surgery
33. Problems with
LMA Insertion
• Failure to press the deflated
mask up against the hard palate
or inadequate lubrication or
deflation can cause the mask
tip to fold back on itself.
34. Problems with
LMA Insertion
• Once the mask tip has started to fold
over, this may progress, pushing the
epiglottis into its down-folded position
causing mechanical obstruction
35. Problems with
LMA Insertion
• If the mask tip is deflated forward it can
push down the epiglottis causing
obstruction
• If the mask is inadequately deflated it may
either
• push down the epiglottis
• penetrate the glottis.
36. INTRAOPERATIVE MANAGEMENT
• Airway patency & correct LMA orientation should be
verified at regular intervals
• Upper abdomen should be periodically observed for
signs of distension
• Deepen the plane of anaesthesia if
laryngospasm/wheezing/ swallowing/ coughing/breath
holding occurs
37. INTRAOPERATIVE MANAGEMENT
• N2O & CO2 can diffuse into cuff thus increasing intracuff
pressure & volume causing airway obstruction
• Cuff Pressure should be monitored periodically with a
pressure gauge or transducer & kept at 60 cm H2O
• LMA can be used for both spontaneous & controlled
ventilations
38. INTRAOPERATIVE MANAGEMENT
• Pressure controlled ventilations with or without PEEP is the mode
of choice for controlled ventilation with LMA because it allows a
lower peak pressure for the same tidal volume with less leak
around the LMA
• In spontaneously breathing patients, pressure support ventilation
improves gas exchange and reduces the work of breathing
39. • The work of breathing can also be reduced by using CPAP
• If regurgitation occurs, 1st sign may be appearance of fluid
travelling up the LMA tube
• In such scenario patient should be placed in head down
position, breathing circuit disconnected and airway tube
suctioned
40. EMERGENCE FROM ANAESTHESIA
• Bite block must be left in place until LMA is removed
• If cuff remains inflated when the LMA i s being removed a
greater mass of secretions is also removed
• LMA should not be removed in the lighter plane of
anaesthesia
• Leaving the LMA in place until the airway reflexes have
recovered and the patient can phonate or open mouth on
command will ensure maintenance of a secure airway
41. • Onset of swallowing is a useful predictor of imminent
wakefulness
• In intra ocular surgeries and in paediatric age group removal of
LMA is recommended in deeper plane of anaesthesia
42. CARE AND CLEANING
• As soon as possible after use the reusable LMA should be
gently cleaned with warm water and a dilute (8-10%)
sodium bicarbonate solution until all visible materials
have been removed
• Mild detergents which doesn’t irritate the mucous
membranes can be used
43. • Pipe cleaner brush can be used to clean the tube
• Inflation valve should not be exposed to any cleansing solution
• Water should not be allowed to enter the cuff
• As much air as possible should be removed from the cuff
shortly before autoclaving
• LMA can be autoclaved at temp up to 135°c (275°F)
• Higher temperature may cause tube to become brittle and
fragment
44. • WHO guidelines and published literatures indicate that
these measures are sufficient for inactivation of
conventional pathogens
• In patients with known or suspected spongiform
encephalopathy it is recommended that LMA be used
and destroyed or LMA unique be used
46. DEAD SPACE
• Dead space with LMA is less than that with face mask
but is greater than with a tracheal tube
• correlation between ETCO2 and arterial CO2 is better
with laryngeal mask than with the face mask and as
accurate as with tracheal tube
• Preferred site for measuring ETCO2 in children is the
laryngeal end of the shaft
47. FLOW RESISTANCE AND WORK OF
BREATHING
• LMA offers lesser resistance than tracheal tube
• But total respiratory resistance and work of breathing are
similar
• LMA flexible has a smaller internal diameter so it imposes
significantly greater resistance than other LMA’s
48. USES OF LMA
• Used in a variety of procedures but best suited for short
procedures making it especially useful for outpatient
procedures
• Maximum duration for LMA use is not known but has
been used for surgeries lasting upto 8 hrs
• Useful in patients with difficult face mask technique
• Useful in difficult or failed intubation
49. • Ophthalmic surgeries
• Tracheal procedures
• Diagnostic and therapeutic fiberoptic laryngotracheoscopy
and bronchoscopy , bronchoalveolar lavage and in placing
bronchial stent
• Useful in trans oesophageal echocardiography
• Various head and neck procedures
• Thyroid surgeries- cuff displaces the gland anteriorly
facilitating surgical access
• Used for carotid endarterectomy
• Congenital conditions
50. • Professional singers and speakers
• Remote anaesthesia
• Supplementing regional blocks
• Out of hospital use especially in toxic mass casualty events
• Obstetrics
• Laser surgeries
• Lower abdominal surgeries
• Neurosurgeries
• Extracorporeal shock wave lithotripsy
51. COMPLICATIONS
• Aspiration of gastric contents
• Gastric distension
• Foreign body entrapped in the LMA tube may get aspirated
or cause airway obstruction
• Airway obstruction due to malpositioning of the cuff
53. ADVANTAGES
• Ease of insertion
• Smooth awakening
• Low operating room pollution
• Avoiding complications of intubation
• Avoiding complications of face mask
• Protection from barotrauma
• Cost effective if used enough number of times
54. DISADVANTAGES
• Relative contraindications like full stomach, previous gastric
surgeries, GERD , diabetic gastroparesis, pregnancy > 14 wks,
dementia.
• Supraglottic pathologies such as cysts, abscess, hematoma.
• Presence of bleeding disorders
• Less reliable airway than the tracheal tube as it may get dislodged
55. Side-Effects of the LMA
• Throat soreness
• Dryness of the throat and/or mucosa
• Side effects due to improper placement vary based on the nature of
the placement
56. CLASSIFICATIONS:
• BASED ON SEALING MECHANISM
1)CUFFED PERILARYNGEAL SEALERS are of two types
• Without directional sealing: LMA, ILMA, Soft Seal LM,
Ambu LM.
• With directional sealing: PLMA.
2)CUFFED PHARYNGEAL SEALERS are of two types
Without esophageal sealing cuff: Cobra-PLA
• With esophageal sealing cuff: LT ,LTS, Combi tube
3)CUFFLESS PRESHAPED SEALERS: SLIPA,I Gel, Baska
Mask
57. • Supraglottic devices are alternatively classified into
generations:
• FIRST GENERATION
• Only with an airway tube
• Seal pressure of 20cm of water
SECOND GENERATION
• With a gastric channel/port for the drain tube
• A seal pressure of more than 30cm of water
• Bite block.
THIRD GENERATION(debatable) In which the mask seal
improves with each positive pressure breath . E.g; Baska mask
58. LMA CLASSIC
• Consists of a curved tube (shaft) connected to an
elliptical spoon shaped mask (cup) at 30° angle
• Two flexible bars at the mask end to prevent the tube
being obstructed by the epiglottis
• Inflatable cuff surrounds the inner rim of the mask
• Black line runs longitudinally along the posterior aspect
of the tube
59.
60. • A 15mm connector at the machine end of the tube
• LMA is made from silicon and contains no latex
• Classical LMA’s are available in 8 sizes
• Significance of the size- too small an LMA will
predispose to gas leaks during positive pressure
ventilation
• Too large an LMA may tend to come up within the mouth
may interfere with procedures in the mouth, may increase
incidence of sorethroat and may even damage the lingual
nerve
61. LMA UNIQUE
• Single use, disposable laryngeal mask airway( d LMA)
• Made up of polyvinyl chloride and costs less than a
reusable LMA
• The dimensions are identical to standard LMA, but tube
is stiffer and cuff less compliant
• Indications- better choice for out of hospital or ward use
Comparisons of the LMA unique with a LMA classic show
little difference in ease of insertion or performance
Intracuff pressure increase with N2o use is significantly less
62.
63. LMA FLEXIBLE
• LMA flexible or wire reinforced LMA ( R-LMA, F-LMA)
• Differs from C-LMA in that it has a flexible wire reinforced
tube
• Tube is longer and narrowed
• Single use version are also available
• They can be bent to any angle without kinking-this allows it
to be positioned away from the surgical field
• Less likely to be displaced during head rotation
64.
65. • Indications- designed for use in surgeries of head &
neck surgeries
• Comparisons between LMA classic reveal that both
are similar in terms of mask position, clinical
performance & pharyngeal mucosal pressures
• Problems- the wire reinforcement doesn’t prevent
obstruction from biting, to avoid this Boyle’s Davis
gag may be used
66. Spiral reinforcing tube may break & cause airway obstruction or
may enter tracheobronchial tree
Small internal diameter limits the size of endoscope or tracheal
tube to be used
Unsuitable if the patient is undergoing MRI
67. LMA FASTRACH
• LMA Fastrach (Intubating LMA or I-LMA) was designed to
overcome some of the limitations of the LMA classic during
tracheal intubation
• Another objective was to eliminate the need to distort the
anterior pharyngeal anatomy in order to visualize the laryngeal
inlet, making the device applicable to patients with history of
difficult intubation & a high or anterior larynx
68.
69. • A single, movable epiglottic elevator bar in place of the 2
vertical bars
• A v-shaped guiding ramp is built into the floor of the mask
aperture to direct the tracheal tube toward the glottis
• The tip is slightly curved to permit atraumatic insertion
• Available in sizes 3,4 & 5
• Both reusable & disposable versions are available
70. • Inserted with the patient in neutral position
• Using head support such as pillow, but no head extension
• Insertion technique consists of one hand movements in saggital
plane
• It doesn’t require placing fingers into the patient’s mouth, thus
minimizing the risk of injury or infection , as well as allowing
insertion from almost any position
71. DESCRIPTION
• It has a short, curved stainless steel shaft with a standard
15mm connector
• Tube is of sufficient diameter that a cuffed 9mm tracheal
tube can be inserted & short enough to allow a standard
tracheal tube cuff to pass beyond the vocal cords
• Metal handle is securely bonded to the shaft near the
connector end to facilitate one handed insertion, position
adjustment & maintain the device in a steady position
during tracheal tube insertion & removal
72. USES
• Designed to facilitate tracheal intubation
• Can also be used as primary airway device
• Useful for anticipated & unexpected difficult airway
• Can be used in children, morbidly obese &
acromegalic patients
73. TRACHEAL INTUBATION
• Tracheal tube recommended with LMA Fastrach is a silicone,
wire reinforced cuffed tube with a tapered patient end & a
blunt tip
• Flexible allowing easier negotiation around the anatomical
curves of the airway
• There is a stabiliser which allows the LMA to be removed
without extubating the patient
74. • It is useful in blind nasal intubation, fiberscope guided & light
stylet guided intubation
• Problems- rigid shaft cannot easily adapt to a change in the
position of patient’s neck
• More likely to be dislodged than LMA classic
• Cannot be used with cases in prone position
• Unsuitable for use in MRI unit
75. LMA C-TRACH
• Similar in construction with LMA Fastrach
• It has 2 built in fiberoptic channels
• Fiberoptic system is sealed & robust, so the LMA C-TRACH
can be autoclaved
• Monitor (viewer) is attached to the LMA C-TRACH by a
magnetic latch connector, it has controls for focussing & image
adjustment
• Available in sizes 3,4 & 5 & is reusable up to 50 times
76.
77. • It is inserted without the viewer attached
• An antifogging solution should be applied to the optical lens
• Viewer is attached after the LMA has been secured & the
patient ventilated
• A real time image of larynx is then displayed
• Useful for satisfactory positioning of the LMA & high first
intubation attempt success rate
78. LMA PROSEAL
• It has 4 main parts- the cuff, inflation line with pilot
balloon, airway tube & drain (gastric access) tube
• All components are made from silicone & are latex free
• Available in 6 sizes
79.
80. • Airway tube of LMA proseal is shorter and smaller in diameter
than that of lama classic and is wire reinforced which makes it
more flexible
• There is a locating strap on the anterior distal tube to prevent
the finger slipping off the tube an to provide an insertion slot for
the introducer tool
• An accessory vent under the drainage tube in the bowl prevents
secretions from pooling and acts as an accessory ventilation por
81. • LMA proseal has a deeper bowl than the LMA classic and does not
have aperture bars
• There is a bite block between the tubings
• Drain tube is parallel and lateral to the airway tube until it enters the
cuff bowl
• When the LMA proseal is correctly positioned the cuff tip lies behind
the cricoid cartilage at the origin of esophagus(superior oesophageal
sphincter)
• It allows the liquids and gases to escape from the stomach
• Gastric tube, Doppler probe, thermometer or medication can be passed
into the esophagus through the drainage port
82. • A plastic supporting ring around the distal drain tube prevents
the tube from collapsing when the cuff is inflated
• LMA proseal has a second dorsal cuff, this pushes the mask
anteriorly to provide a better seal around the glottic aperture
and helps to anchor the device in place(dorsal cuff is not
present on 1.5, 2 and 2.5 proseal)
84. USES
• It can be used for both spontaneous and controlled ventilation
but is more suited for controlled ventilation
• Sealing pressure is higher than LMA classic making it a better
choice where higher airway pressures are required
• Useful for surgical procedures in which intraoperative gastric
drainage or decompression is needed
• Can be used in known cases of difficult airway
• Safe in MRI unit
85. PROBLEMS WITH LMA PROSEAL
• Because of its narrow airway tube it is less useful in
spontaneously breathing patients
• It requires a greater depth of anaesthesia than with LMA classic
• It can cause airway obstruction by compressing the supra glottic or
glottic structures or by cuff infolding
• Relatively contraindicated for intra oral surgeries because it cannot
be easily moved around the mouth
• It has shorter life span than LMA classic
86. LMA SUPREME
• It is a single use version and has clinical utilities similar to that of
LMA proseal
• It has a reinforced tip and moulded distal cuff which prevents
folding
87. LMAAMBU AURA
• It is disposable laryngeal mask with a built in curve that
replicates the natural human anatomy
• It has a soft cuff, reinforced tip to prevent folding and no
epiglottis bar
• It comes in 7 sizes
• It is of two types- ambu aura once, ambu aura 40
88.
89. LMA SOFT SEAL
• It is a clear disposable mask made from polyvinylchloride
• The oval cuff doesn’t taper at the tip
• The inflation tube is attached to the airway tube
• It has no epiglottic bars
• It is available in 7 sizes
• Insertion procedure is similar to that of an LMA
• The cuff is less permeable to N2O than silicon masks. So the cuff
increase pressure is lesser
• It has lower or equal incidence of sore throat compared to C-LMA
92. AMBU LARYNGEAL MASK
• It is a disposable device that has a cuff that is tapered at the tube
• Airway tube is larger and more rigid
• It is available in 7 different sizes
93. INTUBATING LARYNGEALAIRWAY
• It is a reusable device made from silicon with a clear curved
tube and a dark blue oval bowl
• Bowl has a downward tilt to prevent slipping below the
epiglottis
• These are designed to improve the seal and help isolate the
oesophagus
• It is available in 3 sizes
94. LARYNGEAL TUBE AIRWAY
• It is a reusable silicon device that has a single lumen that is closed at the
tip
• Single use versions( LT-D) are made of polyvinylchloride
• Laryngeal tube suction(LTS, Sonda laryngeal tube, SLT) has an
additional oesphageal lumen posterior to the respiratory lumen that ends
distal to the oesophageal cuff for suctioning and gastric tube placement
• Laryngeal tube has a small (oesophageal, distal ) cuff near the blind tip
and a larger (oropharyngeal , proximal) cuff near the middle of the tube
with one inflation tube to inflate both the cuffs
• The airway tube is relatively wide & curved
95. • These allow suctioning of fibre scope passage
• The tube size internal diameter colour coded on the connector,
with each size having a different colour
• Cuffs should be inflated to pressure of 60 cms H2O. The
proximal cuff will fill first & then followed by distal cuff
• It can be used in both spontaneous & controlled ventilations
• It can be used for nasotracheal & oral intubations
• Gas exchange is through two anteriorly facing oval shaped
openings(ventilation holes) between the two cuffs
96.
97. PERILARYNGEALAIRWAY
• Its also known as cobra PLA/CPLA
• It’s a single use plastic device
• It has high volume, low pressure, oval cuff that is shaped to fit in the
hypopharynx at the base of tongue
• It is available in 8 sizes
• Airway sealing pressure is found to be higher & the laryngoscopic view
superior with the cobra PLA compared with classic LMA
• Useful in patients with “difficult to intubate/ ventilate” situations with LMA
classic/ Fastrach failure
• Its disadvantage is that it doesn’t prevent aspiration
98.
99. STREAMLINED PHARYNX AIRWAY
LINER
• The streamlined liner of the pharynx airway – SLIPA it is a
plastic disposable uncuffed device that is anatomically
preshaped to line the pharynx
• It is a supra laryngeal airway device with a hollow structure
that permits the storage of regurgitated liquids thereby
minimizing aspiration risk.
• It is shaped like a hollow boot with a toe, bridge and heel
• There is an anterior opening for ventilation
• End of the toe rests in the oesophageal aperture
100. STREAMLINED PHARYNX AIRWAY
LINER
• Bridge fits into the pyriform fossa
• Heel connects to the airway tube which is rectangular in
shape and has a colour coded connector
• It has a capacity of 15 times the capacity of LMA classic,
about 45-50 ml– 50ml.
• It is available in 6 adult sizes
• As there is no cuff N2O has no effect on sealing pressure
101.
102. OESOPHAGEAL TRACHEAL
COMBITUBE
• The combitube is a single use double lumen that has a unique
design that provides an airway for either esophageal or tracheal
placement.
• It has a large proximal latex oropharyngeal balloon and a distal
oesophageal low pressure cuff with multiple holes in between.
• It is useful in patients in whom neck movement is
contraindicated and in those whose vocal cords cannot be
visualized because of a limited airway or massive bleeding.
105. i-GEL
• Made from a unique, soft, gel-like material to allow ease of insertion
and reduced trauma.
• Gastric channel designed to improve and enhance patient safety.
• Integral bite-block reduces the possibility of airway channel occlusion.
• Virtually eliminates rotation.
• Reduces the possibility of epiglottis downfolding and obstructing the
airway.
• Unique packaging protects the i-gel in transit and ensures that it
maintains its anatomical shape.