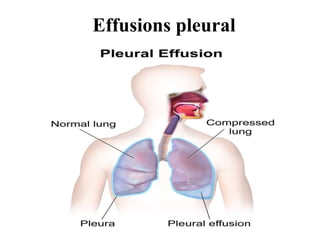
2. Effusions pleural:
• Pleural effusion, also called water on the lung, happens
when fluid builds up in the space between your lungs
and chest cavity. You may have symptoms, such as
chest pain, depending on the cause.
• Thin membranes, called pleura, cover the outside of the
lungs and the inside of the chest cavity.
• There’s always a small amount of liquid within this
lining to help lubricate the lungs as they expand within
the chest during breathing.
• However, if too much fluid builds up, for example,
because of a medical condition, problems can arise.
Doctors call this pleural effusion.
• Various conditions can lead to pleural effusion,
but congestive heart failure is the most commonTrusted
Source cause.
3. Symptoms:
• Some people with pleural effusion don’t have any symptoms.
They may have symptoms of an underlying disease, such as a
cough or fever.
• You may find out you have pleural effusion through a chest X-
ray or physical examination done for another reason.
• When a doctor examines you, they may notice expansion on
one side of the chest and a dull sound when they tap on that
side.
• Depending on the cause, a person with pleural effusion may
also have:
• chest pain
• cough
• fever
• shortness of breath
• See your doctor immediately if you have symptoms of pleural
effusion.
4. Causes and types:
• Pleural effusion happens when fluid accumulates in
the chest cavity outside the lung.
• It can be either transudative or exudative.
• Transudative pleural effusion happens when
increased pressure on the small and large vessels of
various organs causes them to be leaky, resulting in
protein-filled fluid collections. It occurs with
coronary heart disease or cirrhosis.
• Exudative pleural effusion happens when there is
irritation, inflammation, or infection. These can
result in extra fluid production, reduced drainage, or
both.
5. Causes of pleural
effusion includeTrusted Source:
• congestive heart failure
• cirrhosis or poor liver function
• pulmonary embolism, which is caused by a blood
clot and is a blockage in the lung arteries
• complications from open-heart surgery
• pneumonia
• severe kidney disease
• autoimmune diseases, such as lupus and rheumatoid
arthritis
• the use of some medications, such
as methotrexate, phenytoin, or amiodarone
6. • radiation therapy
• rupture of the esophagus
• ovarian hyperstimulation
syndrome
• certain types of cancer for
instance, lung cancer and breast
cancer
• COVID-19
7. Types:
• Pleural effusion can be classifiedTrusted Source as
transudative or exudative.
• Transudative pleural effusions:
• This type is caused by fluid leaking into the pleural
space due to increased pressure in the blood vessels.
• It can happen if you:
• have congestive heart failure
• have cirrhosis
• have kidney disease
• have just started peritoneal dialysis
• have malnutrition due to low albumin levels in the
blood
8. Exudative effusions:
• This happens when a buildup of fluid occurs as the result of:
• inflammation
• infection
• tumors
• a lung injury
• Conditions that could result in this type of pleural infusion include:
• tuberculosis
• cancer
• inflammatory conditions, such as pancreatitis, lupus, or rheumatoid arthritis
• complications from heart surgery
• chylothorax, which results from an obstruction in the lymph vessels
• pneumonia
• hemothorax, when blood collects in the pleural cavity
• Some conditions, such as pulmonary embolism, can lead to either transudate
or exudate pleural effusion.
9. Pleural effusions and cancer:
• Pleural effusions can occur when cancer cells spread to the
pleura or block the flow of normal fluid within the pleura.
Fluid may also build up due to certain cancer treatments, such
as radiation therapy or chemotherapy.
• Certain cancers are more likely to cause pleural effusions than
others, including:
• lung cancer
• breast cancer
• ovarian cancer
• leukemia
• melanoma
• cervical cancer
• uterine cancer
• mesothelioma, which results from exposure to asbestos
10.
11. Signs and symptoms often include:
• shortness of breath
• cough
• chest pain
• weight loss
• The doctor may drain the fluid or carry out pleurodesis if
you’re likely to need repeated drainage. This involves
insering a shunt that redirects the fluid away from the chest.
• They may prescribe antibiotics if you have or are susceptible
to infection. Steroids or other anti-inflammatory medications
may reduce pain and inflammation. They will also discuss
other treatment options for cancer.
• People who are undergoing treatment for cancer may also
have compromised immune systems, making them more
prone to infections or other complications.
12. Treatment:
• The treatment and outcome will depend on the cause of the
pleural effusion.
• Draining fluid:
• One way to treat pleural effusion is by draining the fluid from
the chest cavity, either with a needle or by inserting a small
tube into the chest.
• You’ll receive a local anesthetic before this procedure, which
will make the treatment more comfortable. You may feel
some pain or discomfort at the incision site after the
anesthetic wears off. Most doctors will prescribe medication
to help relieve pain.
• You may need this treatment more than once if fluid builds up
again.
• Other treatments may be necessary to manage fluid buildup if
cancer is the cause of the pleural effusion.
13. Antibiotics:
• If you have a bacterial infection, the doctor will likely
prescribe antibiotics or administer them intravenously.
They will usually do this alongside drainage.
• Pleurodesis:
• Pleurodesis is a treatment that creates mild
inflammation between the lung and chest cavity pleura.
After drawing the excess fluid out of the chest cavity, a
doctor injects a drug into the area. This drug causes the
two layers of the pleura to stick together, which
prevents the future buildup of fluid between them.
• A doctor may decide to do this if pleural effusion is due
to cancer. It reduces the need for frequent drainage.
14. Surgery:
• If symptoms don’t improve with drainage and
antibiotics, the doctor may recommend thoracoscopic
decortication or thorascopic debridement. They will
insert a thoracoscope into the pleural space then either
remove any tissue that is causing a problem
(decortication) or surgically clean a wound to enable it
heal (debridement). A doctor may call thisTrusted
Source a medical thorocoscopy or a pleuroscopy.
• In some cases, a doctor surgically inserts a shunt, or
small tube, into the chest cavity. This helps redirect the
fluid from the chest into the abdomen, where it can be
more easily removed by the body. This may be an
option for those who don’t respond to other treatments.
• Pleurectomy, in which the surgeon removes part of the
pleural lining, may also be an option in certain cases.
15. Diagnosis:
• Your doctor will perform a physical examination and listen to your
lungs with a stethoscope. They may also order a chest X-ray to
help diagnose pleural effusion.
• Other possible tests includeTrusted Source:
• chest ultrasound
• CT scan
• thoracentesis, where the doctor removes some pleural fluid for
analysis
• bronchoscopy
• pleural biopsy
• Thoracentesis involves removing fluid from the pleural membrane
area by inserting a needle into the chest cavity and suctioning the
fluid into a syringe. The doctor will use ultrasound to guide the
needle. At the same time, they may drain the excess fluid from the
chest cavity. The fluid will then be tested to determine the cause.
16. • Your doctor may also choose to perform a pleural
biopsy, which involves taking a tissue sample from the
pleura. They do this by inserting a small needle from
outside the chest wall into the chest cavity.
• If they discover you have a pleural effusion but are
unable to diagnose which type, your doctor may
schedule a thoracoscopy. This is a surgical procedure
that lets the doctor see inside the chest cavity using a
fiber-optic camera.
• For this procedure, your doctor will make a few small
incisions in the chest area while you’re under general
anesthesia. Then they’ll insert the camera through one
incision and the surgical tool through the other to
extract a small amount of fluid or tissue for analysis.
17. Risks and complications:
• Pleural effusions can be complicated or uncomplicated.
Uncomplicated pleural effusions contain fluid without signs of
infection or inflammation. They’re less likely to cause
permanent lung problems.
• Complicated pleural effusions, however, contain fluid with
significant infection or inflammation. They require prompt
treatment that frequently includes chest drainage.
• Pleural effusion can be a sign of severe symptoms with some
diseases. In 2021, some scientistsTrusted Source found that
people with COVID-19 who developed pleural effusion were
more likely to have severe inflammation and complications,
which could affect their chances of recovery.
• Treatment can also lead to complications.
• Minor complications from more invasive treatments can
include slight pain and discomfort, which often go away with
time. More serious complications will depend on the severity
of the condition, the cause, and the treatment used.
18. Serious complications can include:
• pulmonary edema or fluid in the lungs, which can result
from draining fluid too quickly during thoracentesis
• partial collapsed lung
• infection or bleeding
• empyema, when there is pus in the pleural space
• trapped lung, when a layer formsTrusted Source around
the lung that prevents it from expanding
• These complications, while serious, are rare. Your
doctor will help determine the most effective treatment
option and discuss the benefits and risks of each
procedure.
19. Diagnostic investigations
1st investigations
to order
Investigations to
consider
Emerging tests
•posteroanterior and
lateral chest x-ray
•pleural ultrasound
•LDH and protein in
pleural fluid and serum
•red blood cell count in
pleural fluid
More 1st investigations
to order
•pleural fluid
cholesterol level
•thoracic CT scan
•thoracic MRI
•helical CT scan
•More investigations to
consider
•tumor markers in
pleural fluid
•procalcitonin
20. Sugar:
• Pleural fluid analysis is a test that examines a sample of fluid that has been
collected in the pleural space.
• This is the space between the lining of the outside of the lungs (pleura) and
the wall of the chest.
• When fluid collects in the pleural space, the condition is called pleural
effusion.
• Thoracentesis should be performed for new and unexplained pleural
effusions when sufficient fluid is present to allow a safe procedure.
• Observation of pleural effusion is reasonable when benign etiologies are
likely, as in the setting of overt congestive heart failure, viral pleurisy, or
recent thoracic or abdominal surgery.
• Laboratory testing helps to distinguish pleural fluid transudates from
exudates. However, certain types of exudative pleural effusions might
be suspected simply by observing the gross characteristics of the fluid
obtained during thoracentesis.
21. Note the following:
• Frankly purulent fluid indicates an empyema
• A putrid odor suggests an anaerobic empyema
• A milky, opalescent fluid suggests a chylothorax, resulting in
most often from lymphatic obstruction by malignancy or
thoracic duct injury by trauma or surgical procedure
• Grossly bloody fluid may result from trauma, malignancy,
postpericardiotomy syndrome, or asbestos-related effusion
and indicates the need for a spun hematocrit test of the
sample. A pleural fluid hematocrit level of more than 50% of
the peripheral hematocrit level defines a hemothorax, which
often requires tube thoracostomy
• Black pleural fluid suggests a limited number of diseases,
including infection with Aspergillus niger or Rhizopus oryzae,
malignant melanoma, non-small cell lung cancer or ruptured
pancreatic pseudocyst, or charcoal-containing empyema
22. Normal pleural fluid
• Normal pleural fluid has the following
characteristics:
• Clear ultrafiltrate of plasma that originates from the
parietal pleura
• A pH of 7.60-7.64
• Protein content of less than 2% (1-2 g/dL)
• Fewer than 1000 white blood cells (WBCs) per
cubic millimeter
• Glucose content similar to that of plasma
• Lactate dehydrogenase (LDH) less than 50% of
plasma
23. Pleural fluid laboratory findings
• Lights criteria (High protein and LDH = exudate),
determines presence of exudate with protein and LDH
levels
– Pleural fluid protein to serum protein ratio >0.5
– Pleural fluid LDH to serum LDH ratio >0.6
– Pleural fluid level >2/3 of upper value for serum LDH
• Additional criteria – Confirm exudate if results
equivocal
– Serum albumin – pleural fluid albumin <1.2g/dL
•
• Glucose
– Low
• Common: Infection (pneumonia) and malignancy
• Rare: TB, haemothorax, Churg-Strauss
24. Protein:
• LDH level – This is classically high in exudates
– Repeated testing confirms continuation or cessation of
process
• Increasing LDH (ongoing inflammation)
• Decreasing LDH (cessation of process)
• Pleural fluid pH (Low glucose and pH = infection or
malignancy)
– Taken if suspect pneumonic or malignant process (Low
glucose)
– <7.20 with pneumonia…Drain the fluid
– <7.20 with malignancy …Life expectancy 30 days
• Amylase
– Useful if suspect pancreatitis as cause
25. Cell count:
• If exudate is confirmed, further testing required to
evaluate cause of exudate
• Differential cell count (predominance of white cells)
– Neutrophils – PTE, pancreatitis, pneumonia, empyema
– Lymphocytes – Cancer, TB pleuritis
– Eosinophila – Pneumothorax, haemothorax,
asbestosis, Churg-Strauss
– Mononuclear cells – Chronic inflammatory process
• Gram stain and culture and cytology
– Use blood culture bottles and specimen jars – especially if
chronic illness or suspect TB or fungus
– Cytology useful in cases of suspected malignancy
•